Article:
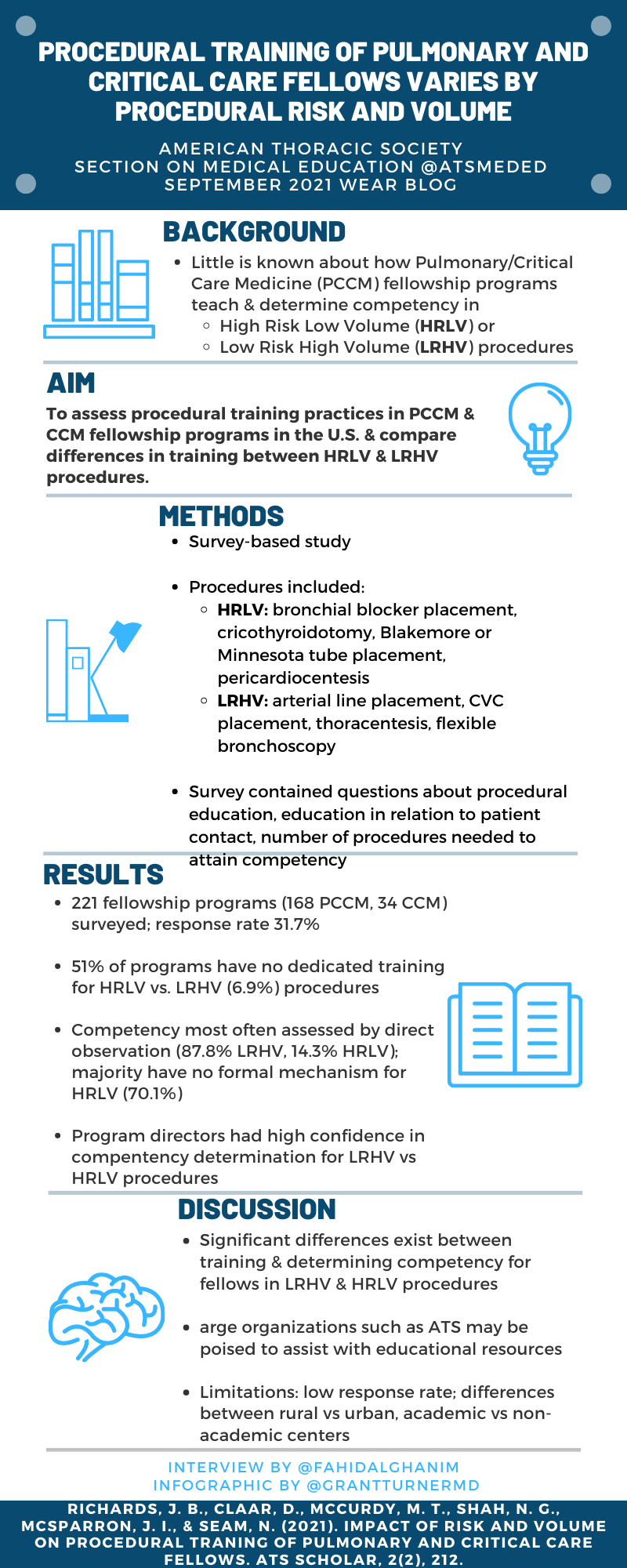
Procedural Training of Pulmonary and Critical Care Fellows Varies by Procedural Risk and Volume
Jeremy B. Richards, Dru Claar, Michael T. McCurdy, Nirav G. Shah, Jakob I. McSparron, and Nitin Seam. Procedural Training of Pulmonary and Critical Care Fellows Varies by Procedural Risk and Volume. ATS Scholar. Published February 11, 2021, as 10.34197/ats-scholar.2020-0110OC
Summary:
Invasive procedures are a core aspect of pulmonary and critical care practice. Procedures performed in the intensive care unit (ICU) can be divided into high-risk, low-volume (HRLV) procedures and low-risk, high-volume (LRHV) procedures. HRLV procedures include cricothyroidotomy, pericardiocentesis, Blakemore tube placement, and bronchial blocker placement. LRHV procedures include arterial line placement, central venous catheter placement, thoracentesis, and flexible bronchoscopy. Despite the frequency and importance of these procedures, little is known about the similarities and differences in procedural training between different Pulmonary and Critical Care Medicine (PCCM) and Critical Care Medicine (CCM) training programs. Dr. Richards and colleagues developed a novel survey tool to assess procedural training of fellows. The survey was sent to 221 fellowship programs, 168 PCCM and 34 CCM, with 70 unique respondents (31.7% response rate). Of the procedural educational strategies assessed, each strategy was used significantly more frequently for LRHV vs. HRLV procedures. Over 50% of respondents reported having no dedicated training for HRLV procedures vs. 7% reporting no dedicated training for any LRHV procedure. For HRLV procedures, almost 77 % of respondents indicated that there was no set number of procedures required to determine competency, vs. 25% for LRHV procedures. For LRHV procedures, fellows were more likely to perform procedures independently without supervision compared to HRLV procedures. Program directors' confidence in their ability to determine fellows' competence in performing procedures was significantly lower for HRLV vs. LRHV procedures. This study highlights the significant differences that exist in procedural training education, competencies and expectations for LRHV vs. HRLV procedures. Increased awareness of this disparity and focused educational interventions may help to bridge this gap.
Interview:
FA: What prompted you to pursue this study? And what were you anticipating to find?
JR: Dr. Nitin Seam, the senior author on our study, and our excellent research team deserve all the credit for conceptualizing this study. In his role as a CCM fellowship program director, Dr. Seam noted that there was a paucity of training opportunities for HRLV procedures in his and other fellowship programs. He brought together our research group and we developed the novel survey instrument used in this study to assess how PCCM or CCM programs taught and assessed various procedures during fellowship training.
Our hypothesis for this study was that there would be significant variation between training and assessment approaches to HRLV and LRHV procedures in fellowship training, and the results confirmed this hypothesis. As such, we weren't surprised by the results as our lived experiences as trainees and educators led us to develop our research question and hypothesis. That said, our hope is that describing and publishing these data will lead to conversations among medical educators and other stakeholders about whether and how to bridge the gaps between LRHV and HRLV procedures in PCCM and CCM fellowship training.
FA: This study showed the significant differences that exist in procedural training education, competencies and expectations for LRHV vs. HRLV procedures. How can we address this gap?
JR: As mentioned above, although our study is primarily descriptive in nature, providing these data about procedural training practices in PCCM and CCM fellowship can hopefully lead to program directors, medical educators, trainees, division chiefs, hospital administrations, and other stakeholders re-considering these aspects of fellowship education. It is important to note that our survey primarily involved academic medical centers (82.6% of respondents), and that generalizations from our results can't be made to training practices in community medical centers (2.9%) or hybrid programs (14.3%). That said, the gap between training for HRLV and LRHV procedures in the academic medical centers included in our study indicates the need for multicenter, collaborative, and constructive strategic planning for addressing this training gap.
FA: Do you think there is a role for ACGME in helping with standardization of procedural training? If so, how?
JR: I think that professional societies such as the American Thoracic Society (ATS) could play a more important role in addressing the training gap between LRHV and HRLV procedures in CCM and PCCM fellowship programs. My personal opinion is that the last thing that program directors and medical educators need is more administrative obligations from accrediting bodies such as the ACGME. Rather than create more paperwork for program directors and medical educators, what would be most beneficial would be to provide well-developed educational resources to help address this training gap, and organizations like the ATS are well-positioned to do this. Developing, assessing, and disseminating resources for helping fellowship programs teach HRLV procedures in an effective and efficient manner seems like the most targeted and streamlined strategy for addressing this educational need.
FA: On a more personal note, how would you approach teaching HRLV procedures to your fellows?
JR: I personally think that a combination of flipped classroom teaching and simulation-based medical education would be the most effective and efficient manner to teach HRLV procedures. The ATS or other organizations could help to develop videos about teaching and learning HRLV procedures such that fellowship directors do not have to develop their own resources – for procedures that occur as rarely as bronchial blocker placement, pericardiocentesis, Blakemore tube placement, or cricothyroidotomy, it would be inefficient and resource-intensive to have each individual fellowship program develop their own educational resources. Rather, having a centralized repository of videos and other teaching resources for programs to use would be an efficient and effective means of providing resources to educators.
Incorporating simulation-based medical education into training for HRLV procedures would be ideal and identifying low-fidelity and low-cost simulators for such procedures would be ideal. It's not reasonable for every PCCM and CCM fellowship program to purchase high cost, high-fidelity simulators to train fellows on these rare (yet high acuity and high stakes) procedures. Rather, innovative and creative medical educators could work to develop and characterize the performance characteristics of lower-fidelity simulation-based teaching experiences for programs to use. Even just spending time familiarizing fellows with the kits for bronchial blocker placement, pericardiocentesis, Blakemore tube placement, or cricothyroidotomy would be of value and go beyond what fellowship programs are reportedly currently doing for teaching their trainees HRLV procedures.
FA: And lastly, are there plans for follow up studies?
JR: Our group, and other medical education researchers, such as Stephanie Maximous at UPMC, are planning follow-up studies both using the existing survey-based dataset as well as developing and assessing the impact of simulation-based medical education interventions for teaching HRLV procedures. We're always looking for collaborators, so if anybody is interested in getting involved in these studies, please don't hesitate to reach out!
Blog post author
Fahid Alghanim, MD, is a third-year pulmonary and critical care fellow at University of Maryland Medical Center. His academic interests include disparities in care for vulnerable populations in the critical care and pulmonary ambulatory setting, acute respiratory distress syndrome (ARDS), palliative care and communication in the intensive care unit, and medical education.
Twitter: @fahidalghanim
Article author

Jeremy Richards, MD, MA, both teaches at Harvard Medical School and is a member of the Beth Israel Deaconess Medical Center (BIDMC) faculty in the Division of Pulmonary, Critical Care and Sleep Medicine. He is a Clinician Educator involved in both undergraduate (UME) and graduate medical education (GME). Clinically, Dr. Richards works in the Medical Intensive Care Units (MICUs) at BIDMC. Among his formal roles in medical education, he is also a core faculty member in the first-year medical school curriculum for a comprehensive course about fundamental basic science and clinical concepts in Pulmonary, Cardiology, and Hematology. He has won numerous awards at Harvard Medical School and BIDMC for his teaching and mentoring abilities. His specific research interests include curiosity in medical learners, critical thinking, cognitive biases, and clinical reasoning in medical education and clinical practice. He has designed, implemented, and published several studies involving these cognitive and perceptual aspects of learning and thinking about medical practice and clinical problems.
Twitter: @jbricha1


