Authors: Fabio Pitta1, Lorena P. Schneider1, Karina C. Furlanetto1,2.
1Laboratory of Research in Respiratory Physiotherapy, Department of Physiotherapy, Universidade Estadual de Londrina, Brazil.
2Research Center in Health Sciences, University of Northern Parana, Londrina, Brazil.
For a long time, physical activity has been one of the main focus for research in chronic obstructive pulmonary disease (COPD), and only in recent years the eyes of the scientific community of this field have also turned to sedentarism. As currently understood, physical inactivity and sedentary behaviour (SB) are not synonyms. Being physically (in)active refers to achieving (or not) a recommended amount of physical activity (PA), generally that proposed by the American College of Sports Medicine (ACSM), i.e., at least 30 minutes/day of moderate-to-vigorous physical activities (MVPA) in bouts of at least 10 minutes, during at least 5 days of the week, or 20 minutes in vigorous activity at least 3 times/week1. Moreover, ACSM recommendations also suggest that individuals with worse physical condition can perform PA bouts shorter than 10 minutes when presenting difficulty to perform it continuously. On the other hand, sedentarism has two most common definitions: one based solely on low intensity PA (activities performed at an intensity <1.5 metabolic equivalent of task [MET]) and another which combines low intensity PA (≤1.5MET) with large proportion of the day spent in the seated or reclined posture2. Therefore, being sedentary refers to spending most of the day in activities requiring minimal energy expenditure or sitting/lying, regardless whether the subject has achieved or not the minimum recommended MVPA3-5. The ranges for intensity of (in)activity and sedentary behavior are illustrated in figure 1. Interestingly, it is possible to be physically active and sedentary at the same time (Figure 2)5-6.
As more attention has been recently given to sedentary behavior and its differentiation from physical inactivity, new studies in COPD have provided interesting information. As an example, it was shown that patients combining two positive characteristics (i.e., physically active and non-sedentary) had better clinical profile than others, reinforcing the message to focus on being both physically active and non-sedentary as the optimal goal for patients with COPD7. On the other hand, avoiding sedentarism (even in an inactive patient) or avoiding inactivity (even in a sedentary patient) present some benefits, whereas patients combining two negative characteristics (physically inactive and sedentary) present the worse clinical profile7. Furthermore, sedentary behaviour was shown to be strongly and negatively correlated with MVPA (r=-0.72) and with time spent in light activities (r=-0.81)(Figure 3)7. It is important to notice that accumulating MVPA leads to important health benefits in the general population, however interrupting longer periods of sedentary behavior with any mild or moderate intensity may also be beneficial1,8. In fact, strategies to increase light intensity PA rather than focusing solely on increasing MVPA are a novel feature in the literature3,9.
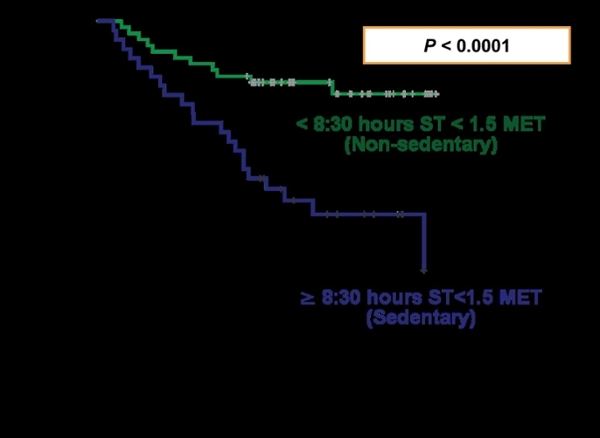
As a final reasoning, there is a considerable body of evidence showing that a more preserved physical activity level is associated with reduced hospital admission10 and longer survival10-13. However, a study from our laboratory14 recently showed that sedentary behavior was also an independent predictor of mortality in subjects with COPD, even adjusting for moderate-to-vigorous physical. This suggests that time to death is shorter in those patients who spent more time in sedentary postures (ie, sitting or lying + sitting) (Figure 4).
In summary, sedentary behavior is not a synonym of physical inactivity and must be avoided at all cost in patients with COPD since it has a markedly negative prognostic value in this population.
References:
-
Garber CE, Blissmer B, Deschenes MR, et al. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med Sci Sports Exerc. 2011;43(7)1334–1359.
-
Gibbs BB, Hergenroeder AL, Katzmarzyk PT, Lee IM, Jakicic JM. Definition, Measurement, and Health Risks Associated with Sedentary Behavior. Med Sci Sports Exerc. 2015;47(6):1295–1300.
-
Hill K, Gardiner PA, Cavalheri V, Jenkins SC, Healy GN. Physical activity and sedentary behaviour: Applying lessons to chronic obstructive pulmonary disease. Intern Med J. 2015;45(5):474–482.
-
Cavalheri V, Straker L, Gucciardi DF, Gardiner PA, Hill K. Changing physical activity and sedentary behaviour in people with COPD. Respirology. 2016;21(3):419–426.
-
Tremblay MS, Colley RC, Saunders TJ, Healy GN, Owen N. Physiological and health implications of a sedentary lifestyle. Appl Physiol Nutr Metab. 2010; 35(6):725-740.
-
Owen N, Healy GN, Matthews CE, Dunstan DW. Too much sitting: the population health science of sedentary behavior. Exerc Sport Sci Rev. 2010; 38(3):105-113.
-
Schneider LP, Furlanetto KC, Rodrigues A, Lopes JRR, Bertoche M, Oliveira L, Hernandes NA, Pitta F. Sedentary behavior and physical inactivity in patients with COPD: two sides of the same coin. In: European Respiratory Society (ERS) International Congress, 2017, Milan. Eur Respir J, 2017; 50: 3690.
-
Healy GN, Matthews CE, Dunstan DW, Winkler EA, Owen N. Sedentary time and cardio-metabolic biomarkers in US adults : NHANES 2003-06. Eur Heart J. 2011;32(5):590–597.
-
Mesquita R, Meijer K, Pitta F, Azcuna H, Goërtz YMJ, Essers JMN, Wouters EFM, Spruit MA. Changes in physical activity and sedentary behaviour following pulmonary rehabilitation in patients with COPD. Resp Med. 2017;126:122-129.
-
Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Antó JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax. 2006; 61(9):772-778.
-
Waschki B, Kirsten A, Holz O, et al. Physical Activity Is the Strongest Predictor of All Cause Mortality in Patients With COPD. Chest 2011; 140(2):331–342.
-
Garcia-Rio F, Rojo B, Casitas R, Lores V, Madero R, Romero D, et al. Prognostic value of the objective measurement of daily physical activity in patients with COPD. Chest 2012;142(2):338-346.
-
Vaes AW, Garcia-Aymerich J, Marott JL, Benet M, Groenen MT, Schnohr P, et al. Changes in physical activity and all-cause mortality in COPD. Eur Respir J 2014;44(5):1199-1209.
-
Furlanetto KC, Donária L, Schneider LP, Lopes JR, Ribeiro M, Fernandes KB, Hernandes NA, Pitta F. Sedentary Behavior Is an Independent Predictor of Mortality in Subjects With COPD. Respir Care. 2017;62(5):579-587.
Figure 1
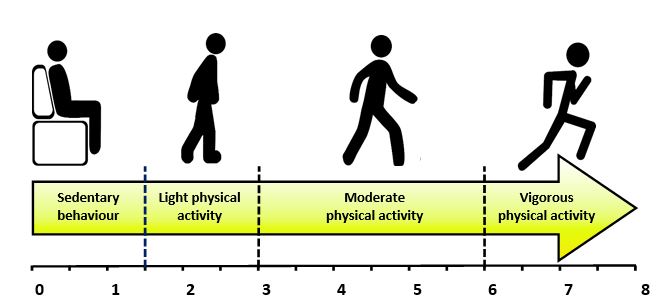
Adapted from Hill et al. (2015)3
Figure 2
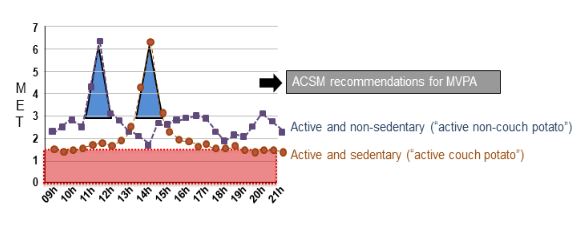
ACSM: American College of Sports Medicine; MVPA: moderate-to-vigorous physical activity; MET: metabolic equivalents of task. Adapted from Tremblay et al. (2010)5
Figure 3
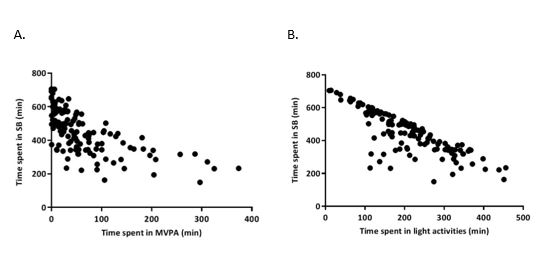
Figure 3. Correlation of time spent in sedentary behavior (SB) and time spent in moderate-to-vigorous physical activities (MVPA) (A) and light activities (B) in patients with COPD. Adapted from Schneider et al. (2017)7
Figure 4