Authors: Linzy Houchen-Wolloff PhD.
Senior Research Associate and Therapy Research Lead,
University Hospitals of Leicester NHS Trust, Leicester, UK.
ATS Planning Committee and Web Committee
The worldwide spread of the SARS-CoV-2 (COVID-19) virus has had a profound effect on healthcare delivery and how we do research, across the globe. This short BITE outlines the research which is taking place in the United Kingdom (UK) to tackle this novel disease and the impact this has had on Pulmonary Rehabilitation (PR) services and research programmes.
The National Institute for Health Research (NIHR) in the UK has fast-tracked the approval processes for COVID-related studies in the National Health Service (NHS). New studies are being added all of the time but there are currently 40 urgent public health studies which are listed as recruiting/ in set up phase on the NIHR website as of 19/05/2020: https://www.nihr.ac.uk/covid-studies/
These comprise a mixture of interventional, observational and pre-clinical studies. At the University Hospitals of Leicester NHS Trust, we have been involved with the following studies:
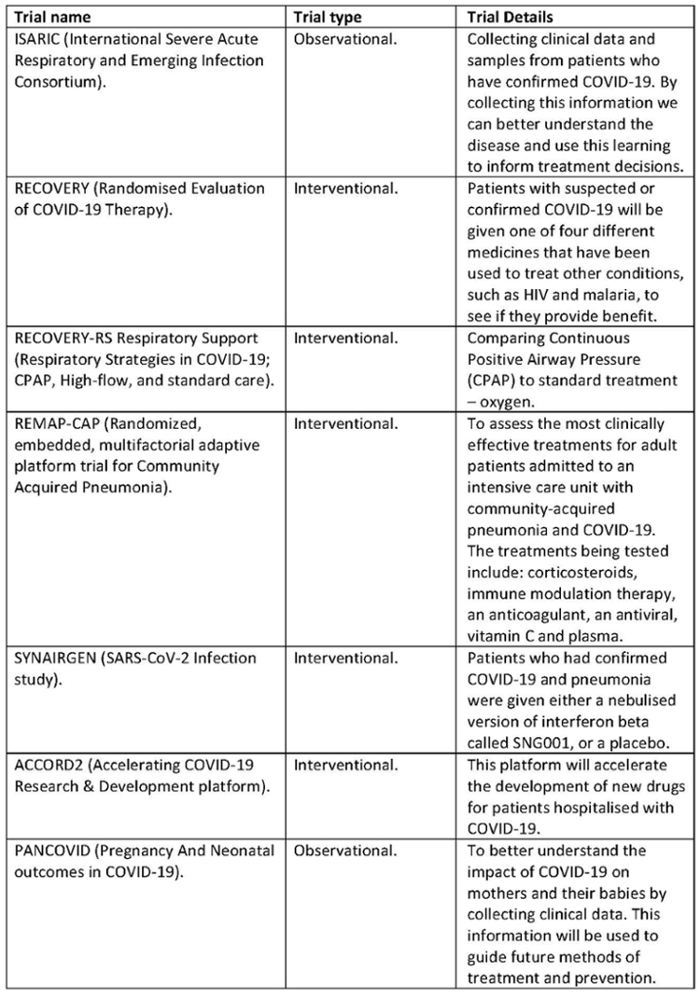
More details on the above trials and links to the study websites can be found at: https://www.leicestersresearch.nhs.uk/about-us-2/covid-19-and-clinical-research/covid-19-trials/ Doctors, Nurses and Therapists who work in PR Research have taken roles in these trials including taking consent, delivering interventions, collecting outcome measures and data entry. Staff and patients in our hospitals have been highly receptive to engaging in COVID research as awareness of the potential impact has increased with pressure from the Chief Medical Officers of England and the devolved nations: https://www.nihr.ac.uk/documents/news/the-importance-of-COVID-19-clinical-trials.pdf A particular focus on recruiting people from Black and Ethnic Minority (BME) groups has been made, in light of findings which show that people from these ethnic groups are the most likely to be badly affected by the disease. A BME call to action has been launched and public campaign messages have been translated into several languages to encourage diversity in research recruitment for COVID https://bepartofresearch.nihr.ac.uk/COVID-19-Research/COVID-19-for-BAME-communities/
The way in which COVID-related studies are being prioritised is quite remarkable. The trials are being designed to be as simple as possible, to reduce any extra burden on the NHS and research sponsors/ ethics committees have put none COVID work to the back of the queue. The impact of COVID-19 on rehabilitation research that was taking place at the time the pandemic hit has been huge. Clinical services rightly take priority over research activity and therefore most current trials were put on hold or managed virtually in order to make quick and effective strategies for the clinical management of COVID-19. Many research staff (doctors, nurses and therapists) were also redeployed to acute areas to support clinical teams. When suspended studies will be able to restart is a careful balancing act. Decisions will need to be made in collaboration with the study sponsors, funders, chief investigators, principal investigators and specific sites. How to restart is complex and subject to conditions that must be met prior to restarting research which include viability, safety and capacity: https://www.nihr.ac.uk/documents/restart-framework/24886#Preconditions
In addition to the urgent public health studies and building upon the initial rapid funding round for COVID-19 research, the NIHR and the UKRI (UK Research & Innovation) are holding a rolling funding call for research into COVID-19. The call is for UK-led academic, small and medium enterprise (SME) and wider industry research that will address a wide range of COVID-19 knowledge gaps, and which will lead to a benefit in UK and potentially international, public health within 12 months. The size of grants will vary according to the needs of each research project, but will need to provide a robust case for value for money. https://www.nihr.ac.uk/funding/covid-19-rapid-response-rolling-call/24650. One might imagine that post-COVID rehabilitation research could fit into this brief. However current social distancing and shielding measures taken in many countries to suppress transmission of the virus have had a dramatic effect on the provision of PR services. Traditionally PR is delivered with a face to face assessment followed by groups of patients attending a rehabilitation class. This is currently not possible but the need for PR has not gone away and consideration is under way about how best to provide effective therapy in the context of the current crisis and beyond. As we start to see not only our traditional chronic respiratory disease patients, but also the wave of people who have had COVID, we anticipate that rehabilitation will be needed more than ever.
COVID-19 has focussed the PR community to shift to remote ways of working and guidance has been issued by some professional bodies on how best to do this (eg. Chartered Society of Physiotherapy: https://www.csp.org.uk/news/coronavirus/clinical-guidance/face-face-or-remote-consultations/guidance-england. The British Thoracic Society (BTS) have also produced resource packs to support remote PR assessments and classes: https://brit-thoracic.org.uk/about-us/covid-19-information-for-the-respiratory-community/. However there is an anxiety amongst PR providers about the effectiveness of remotely provided programmes and how to prescribe exercise safely when we have not completed a face to face assessment, with particular concerns about cardiovascular stability and oxygen desaturation. These parameters can clearly only be measured remotely if patients have access to specific monitoring equipment. Similarly, we can expect patients to worry about attending group sessions because of cross-infection risks, which may amplify already low levels of uptake to PR.
The requirement to rapidly change how we ‘do’ rehabilitation in response to the pandemic is likely to change the face of PR forever. To this end, the ATS PR Assembly planning committee has plans to share ideas and data on this and a Journal Club is also being planned by the ATS PR web committee to facilitate discussions on how we are conducting PR across the globe.


