Obstructive Sleep Apnea Case Study
Shirin Shafazand, MD, MS
Neomi Shah, MD
for the Sleep Education for Pulmonary Fellows and Practitioners,
SRN ATS Committee
Part 1: Case Presentation
Mr. Simon Applegate (SA) is a 55 year old male who comes to your office with complaints of shortness of breath. He has gained 10 lbs over the past 6 months and feels that his breathing is more difficult when walking up a flight of stairs. There has been no cough or sputum production and he has no other respiratory complaints. He is here at the insistence of his wife and feels that he will probably be back to normal if he loses the extra weight. He has a history of childhood asthma but has not had any exacerbations as an adult. His past medical history is also relevant for hypertension, recently diagnosed non-insulin-dependent diabetes, and hyperlipidemia. His is an ex-smoker and quit 10 years ago with a 10 pack-year history of smoking. He works as a bank executive and is married with 2 children. He denies any occupational exposures.
His wife, who accompanies him on this visit, mentions that he has been more tired lately when he comes home from work and has trouble concentrating on tasks. She often finds that he has dozed off in front of the TV while waiting for dinner. He has restless sleep during the night, and she is getting tired of having her own sleep disrupted with his loud snores. He does little else but sleep during the weekend and she worries that might be a sign of depression.
Questions
- What are important components of a good sleep history?
- What is the differential diagnosis of daytime hypersomnolence?
- What are available tools to measure daytime hypersomnolence?
Case Presentation
Upon further questioning, SA admits that he has been more sleepy as of late. He has, on occasion, fallen asleep during meetings, and much to his embarrassment, colleagues nudge him awake when his snoring starts. He goes to bed around 11 pm, falls asleep quickly, but may wake up several times throughout the night to go to the bathroom. He wakes up at 7 am to get ready for work and has to drag himself out of bed. His Epworth sleepiness score (ESS) is 12 out of 24. He doesn’t take any scheduled naps during the week but tries to catch up during the weekends by sleeping in and taking afternoon naps. He has not been in any car accidents due to sleepiness. He drinks 2 cups of coffee in the morning and several caffeinated sodas throughout the day.
His physical exam is remarkable for blood pressure of 150/70, oxygen saturation of 95% on room air, body mass index of 35 kg/m2, Mallampati score III, high arched palate, and neck size 17.5 inches (44.5 cm). Respiratory, cardiac, and abdominal examination are otherwise unremarkable.
Questions
- What are important components of a good sleep physical examination?
- What are risk factors for obstructive sleep apnea (OSA), in general, and this patient in particular?
- What are symptoms of OSA?
- What questionnaires can be used to better quantify risk for OSA(pre-test probability)?
Part II: Diagnostic Testing
You decide that SA is at high risk for OSA and request in-lab, attended polysomnography. The sleep study report is as follows:
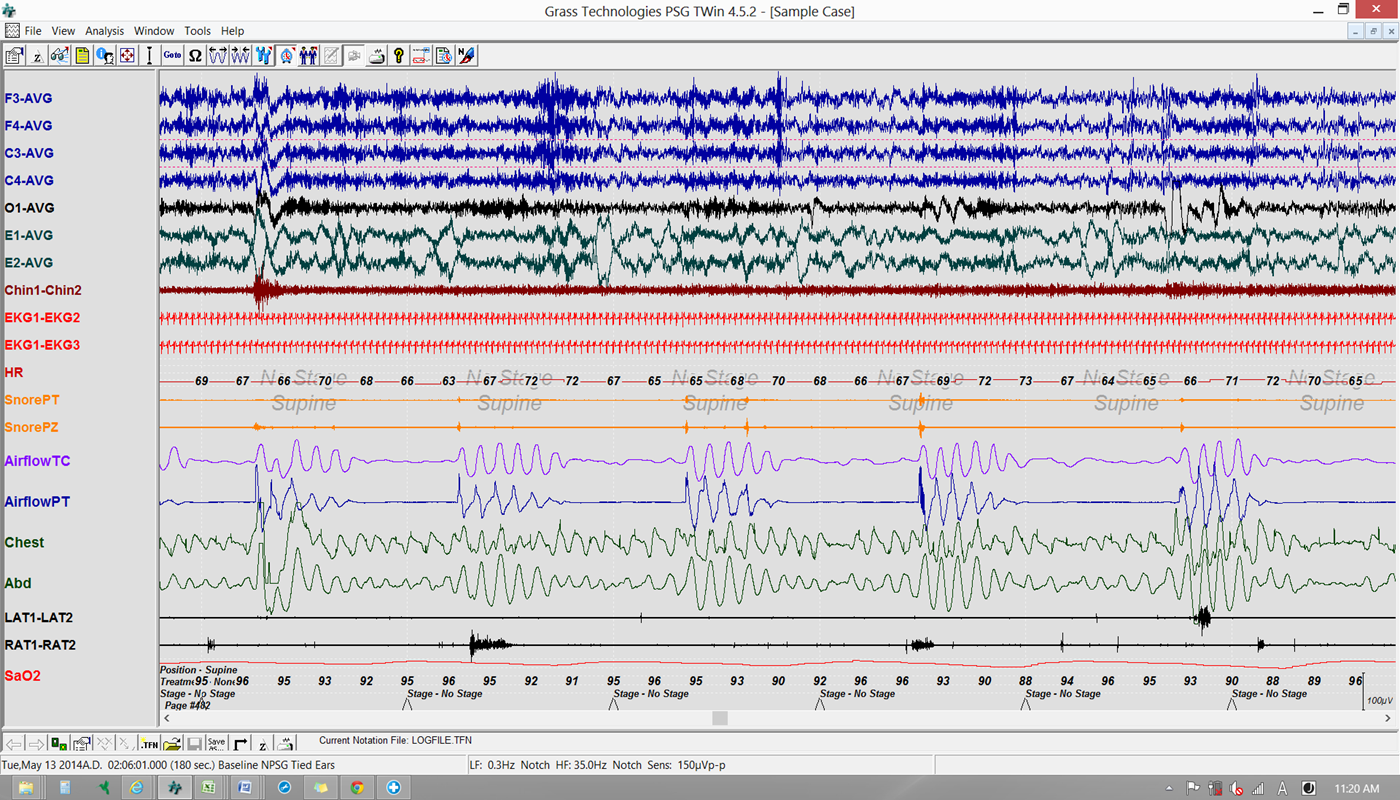
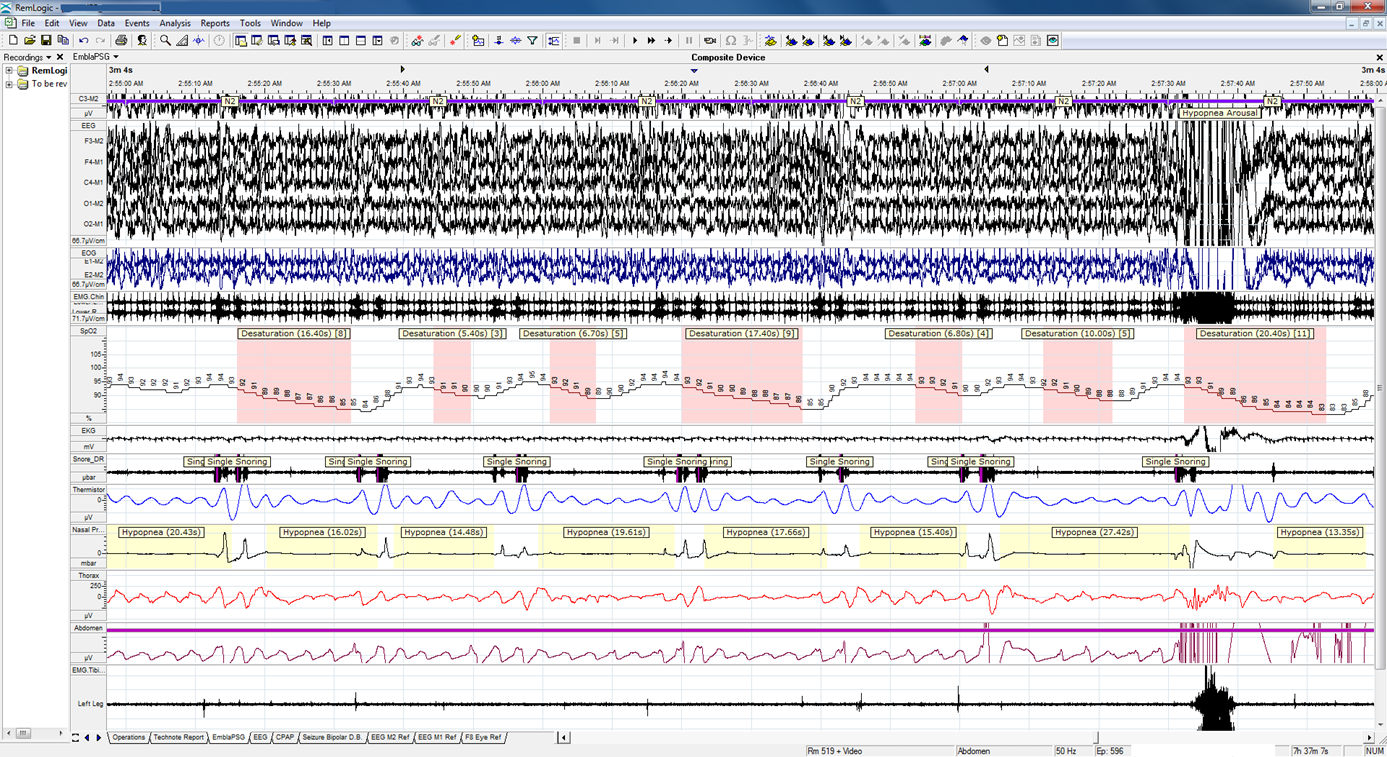
SLEEP ARCHITECTURE: (frontal, central and occipital EEG, right and left EOG and digastric EMG) The exam started at 22:17 and ended at 05:39. Sleep latency was 10 minutes, and REM Latency was 85 minutes. Total sleep time was 404.3 minutes with a sleep efficiency of 91.5 %. The sleep stage distribution showed stage N1 ( 16.7%), stage N2 ( 67.3%), stage N3 ( 0 %), and REM sleep (16 %). The total amount of wake after sleep onset (WASO) was 35.5 minutes and there were 236 arousals during the exam.
RESPIRATION: There were 295 respiratory events consisting of 35 obstructive apnea(s), 22 mixed apnea(s), 0 central apnea(s), 238 hypopneas and 0 respiratory effort-related arousals (RERAs). The AHI during REM sleep was 23.1. The average event duration was 27.3 seconds, and the maximum duration was 55.2 seconds. The supine and non-supine RDI were 75.3 and 41.2 respectively.
OXYHEMOGLOBIN SATURATION: (pulse oximetry with beat by beat sampling) Mean oxyhemoglobin saturation was 94.7%. Oxyhemoglobin saturation was below 88% for 2 minutes. The SaO2 ranged from 86% to 99%. The patient was studied on room air.
Tracings
Questions
- What tests are available to diagnose OSA?
- What are practice guideline recommendations for the use of portable sleep studies? How do you calculate AHI and RDI? What is the AHI and RDI for this patient?
- What is the difference between obstructive and mixed sleep apnea and what are clinical implications of such a distinction? How do you classify severity of sleep apnea?
- What is the sleep apnea severity in this case?
Part III: Treatment
Based on polysomnography results you make treatment recommendations.
SA asks whether there is a relationship between sleep apnea and his recent diagnoses of high blood pressure and diabetes. He also wants to know what impact if any will treatment have on his health.
Questions
- What treatment options are available for OSA and what would you recommend for this patient?
- Is OSA associated with long term health outcomes?
- What is the strength of the evidence? What are proposed mechanisms for the association between OSA and cardiovascular outcomes (hypertension, MI)?
Part III: Treatment
After some discussion, SA accepts your recommendations and opts for CPAP therapy.
You arrange for in-lab CPAP titration and after reviewing the results, you prescribe CPAP at 12 cmH20 and a medium-size full-face mask.
Questions
- What are potential advantages and disadvantages to using auto-PAP devices vs. in-lab PAP titration?
- What is PCrit?
- What is the impact of CPAP therapy on sleep apnea health outcomes?
- What are predictors of short term and long term CPAP compliance?
Conclusion
SA returns after 3 months of cpap use and reports improvement in daytime hypersomnolence. He has been paying attention to his diet and has been exercising more with a 10 lb. weight loss. He wonders whether he still needs CPAP.
He reports nightly use of at least 5 hours with initial difficulty tolerating the mask but gradual increase in tolerance. He uses a humidifier and that has helped somewhat.
Questions
- What are usual follow-up recommendations for newly diagnosed sleep apnea?
- What is the impact of weight loss on OSA?
- How is CPAP compliance measured and what is considered good compliance?
Download the Facilitator Guide.
Download case in PowerPoint or PDF.
Please complete the online survey and download your certificate.


