Contributed by Hillary Loomis-King, MD and James A. Rowley, MD, Wayne State University School of Medicine Detroit, MI
- 51 yo with ALS presenting with 2 pillow orthopnea and progressive dyspnea.
- Sleep history positive for awakenings at night with shortness of breath and morning headaches. No snoring or gasping.
- Daytime fatigue and sleepiness with Epworth = 10.
- A PSG was performed.
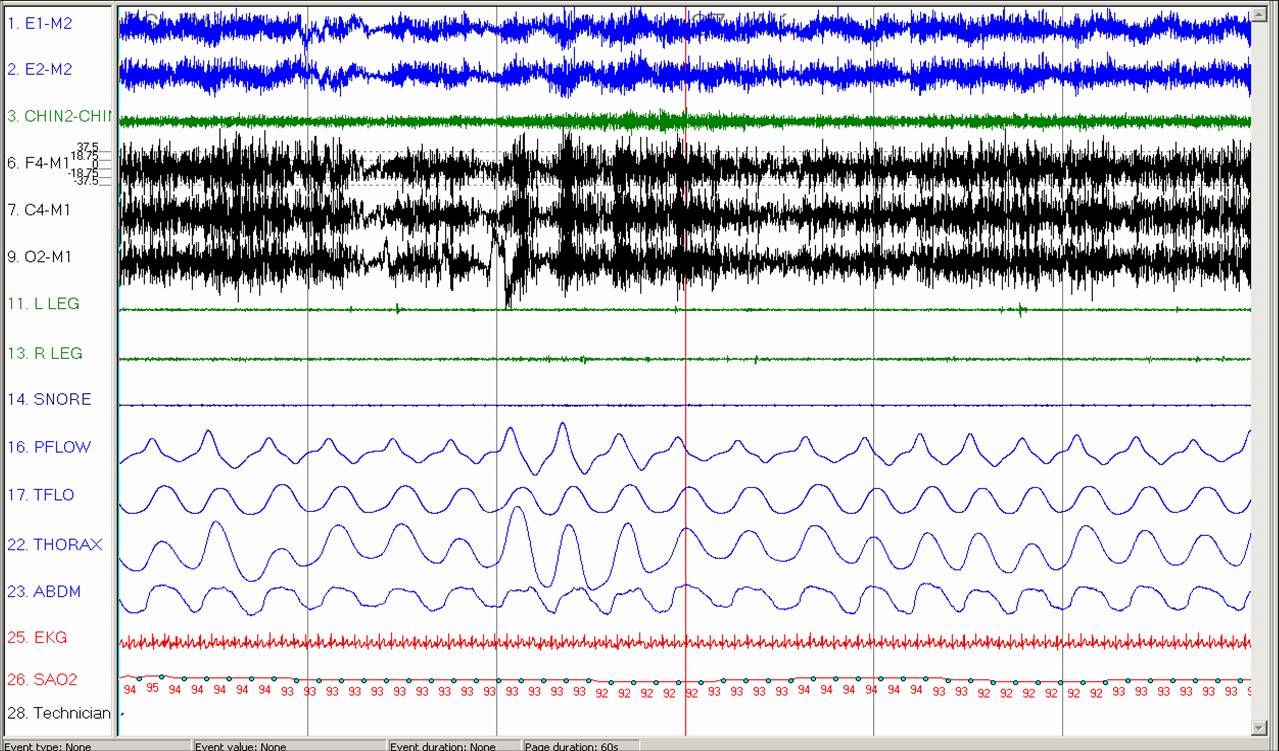
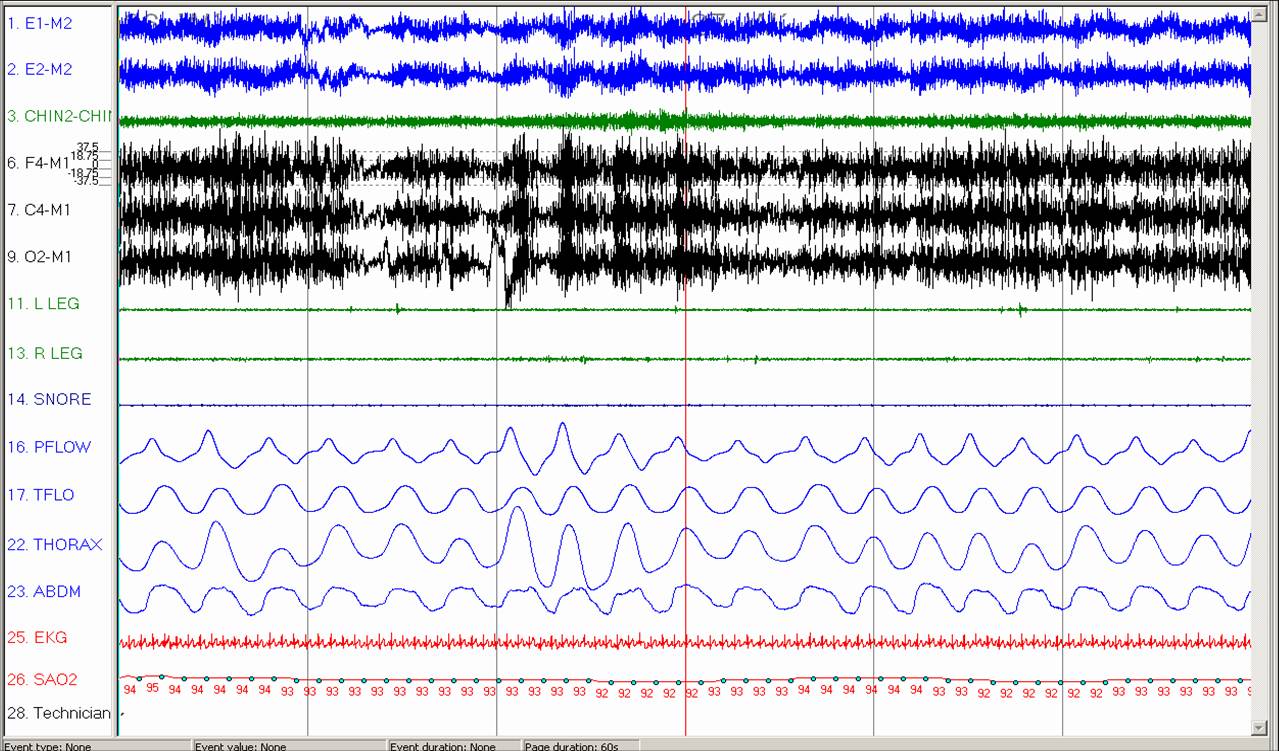
- The first fragment shows a 1 minute segment of wakefulness; the second fragment shows a 1 minute segment of stable Stage N3 sleep.
Question #1: What abnormal finding noted is consistent with sleep disordered breathing in this patient?
Question #2: What additional daytime study can be performed that would confirm the etiology of this abnormal finding?

Answer #1: Paradoxical breathing
In the first fragment during wakefulness, the thorax and abdomen are moving in synchrony (blue double arrows) while during Stage N3 sleep (second fragment, green double arrows), the thorax and abdomen are moving paradoxically and there is oxyhemoglobin desaturation to 88%.
This finding is consistent with diaphragm dysfunction.
In addition to the paradoxical breathing shown, the patient exhibited severe obstructive sleep apnea with AHI 30/hr; all of the respiratory events were hypopneas and were primarily in the supine position and during transitions between wakefulness and N1 sleep.
Answer #2: Sitting and supine spirometry.
Diaphragm dysfunction can be confirmed by performing sitting and supine spirometry. In normal subjects, the supine position results in a ~10% drop in volumes. In diaphragm dysfunction, spirometric lung volumes decrease as much as 50% as the patient goes from a sitting position to a supine position.
For this patient, sitting FEV1 and FVC were 1.07L and 1.40L respectively. In the supine position, FEV1 and FVC decreased to 0.6L and 0.89L respectively, consistent with the diagnosis of bilateral diaphragm dysfunction.
Arnulf, et al. investigated 21 ALS patients, 13 (Group 1) with evidence of diaphragm dysfunction (presence of paradox, respiratory pulse [visible inspiratory contraction of the inspiratory neck muscles] or absence of diaphragm response to stimulation). Group 2 patients had no evidence of diaphragm dysfunction.
Slow vital capacity was significantly lower in Group 1 (61% v. 86% of predicted). No other pulmonary function test parameters differed between the 2 groups.
Group 1 patients had less REM sleep and more wake after sleep onset than Group 2 patients. Otherwise, sleep architecture was similar between the two groups.
There was no difference in the AHI between the two groups.
Finally, there was reduced median survival with diaphragm paralysis: survival was 217 days in group 1 versus 619 days in group 2.
The plan is to treat this patient with positive airway pressure therapy, likely bi-level. However, the patient has not returned for the titration study at the time of this writing.
References
- Ferguson KA, et al. Sleep-disordered breathing in amyotrophic lateral sclerosis. Chest 1996; 110:664.
- Arnulf I, et al. Sleep disorders and diaphragmatic function in patients with amyotrophic lateral sclerosis. Am J Respir Crit Care Med 2000; 161:849.