Contributed by Ziad S. Shaman, Assistant Professor of Medicine, Case Western Reserve University, Division of Pulmonary, Critical Care and Sleep Medicine, MetroHealth Medical Center
Metronomic apnea
Ziad S. Shaman, Assistant Professor of Medicine, Case Western Reserve University, Division of Pulmonary, Critical Care and Sleep Medicine, MetroHealth Medical Center
A 50 year old man presented with snoring, witnessed apneas, unrefreshing sleep, and excessive daytime sleepiness (ESS 17) despite adequate sleep duration. The patient had history of hypertension (well controlled with amlodipine and hydrochlorothiazide) and a seizure disorder that was difficult to treat. The patient continued to have seizures (about twice a week) while taking phenytoin, lamotrigine, and levetiracetam. A vagal nerve stimulator (VNS) was implanted 1 year prior to presentation resulting in reduction of seizure frequency to twice per month. The patient denied history of heart rhythm problems. His BMI was 32.5 kg/m2. He had a crowded oropharynx, mildly congested nasal mucosa and a healed surgical scar on the upper left chest, in the area of VNS implantation. The cardiopulmonary exam was otherwise unremarkable. Frequently, during the interview, the patient seemed to stop speaking abruptly to clear his throat.
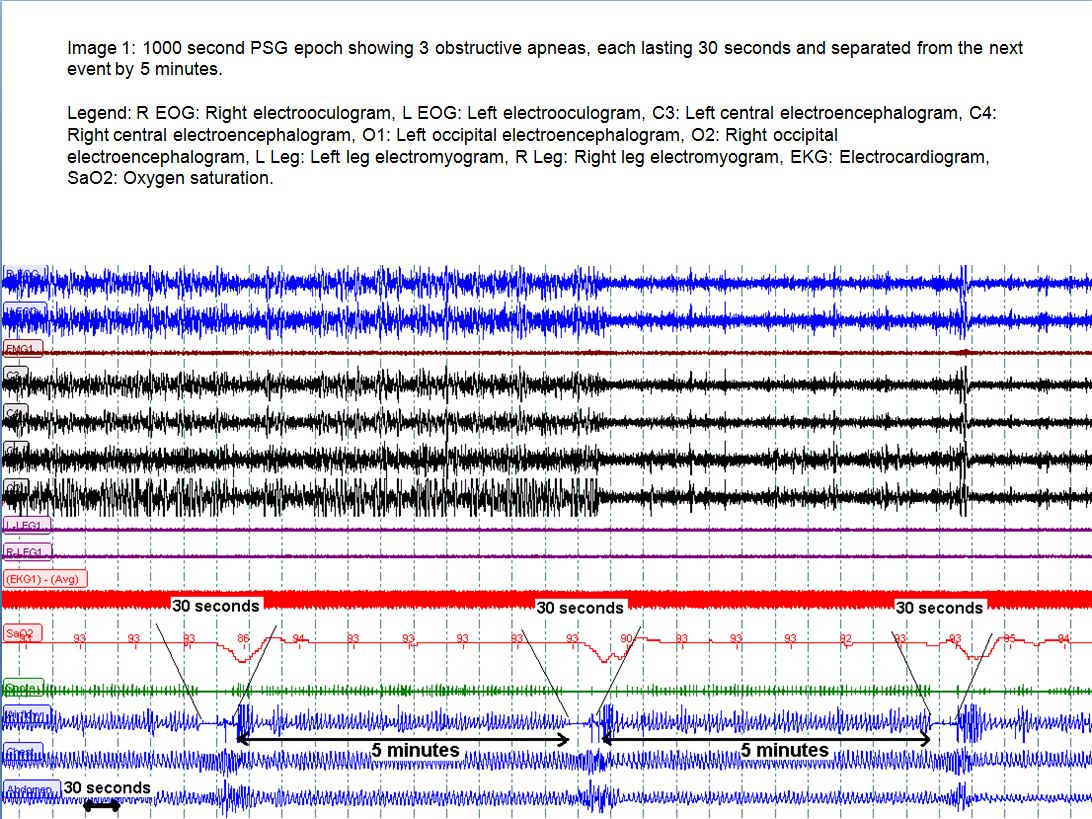
A polysomnogram confirmed the presence of mild obstructive sleep apnea (Apnea/Hypopnea Index 13.5). However, the respiratory events were unusually rhythmic and occurred with the accuracy of a metronome. Every respiratory event lasted exactly 30 seconds, and was separated from the next event by 5 minutes
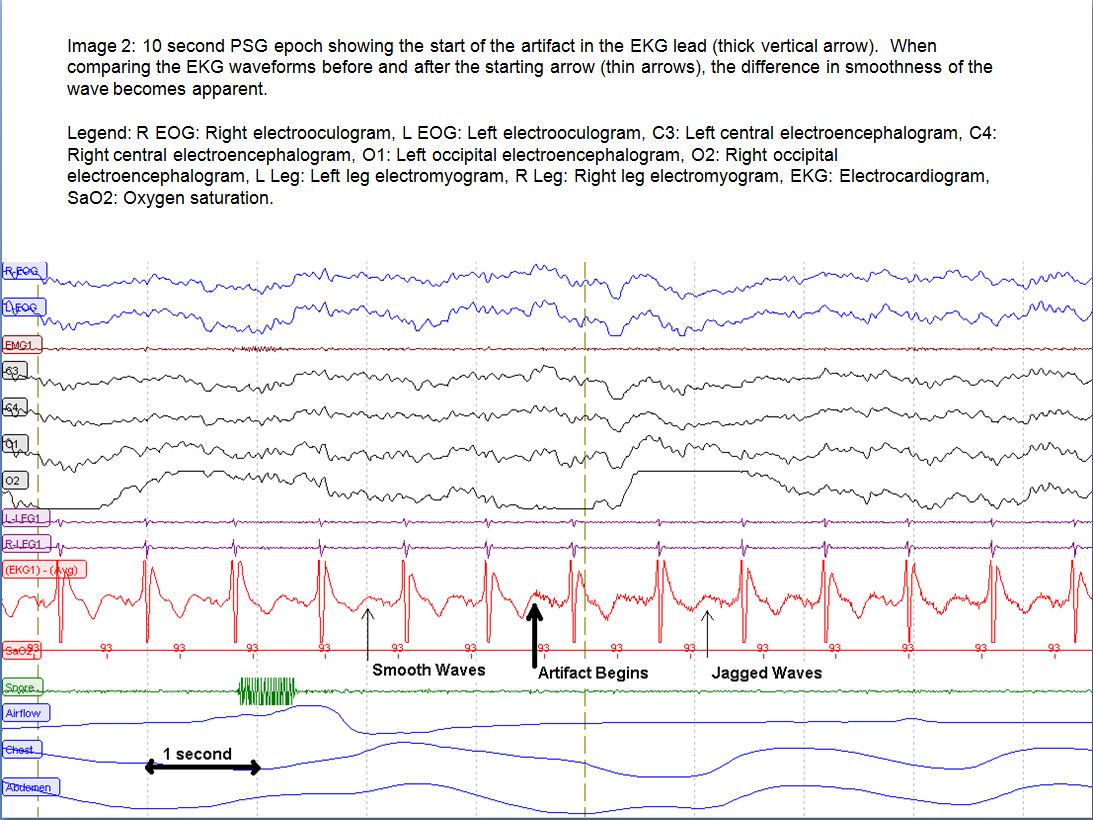
Upon careful examination of the polysomnographic signals, and after removal of high pass filters, a fine artifact of high frequency was seen on the electrocardiogram wave, making it appear jagged, intermittently. The artifact occurred in bursts, each lasting 30 seconds. The occurrence of this artifact coincided exactly with the patient’s respiratory events.
Questions:
- What is the cause of the electrocardiogram artifacts?
- Myocardial fiber stretch during episodes of apnea.
- Electrical activations of the implanted VNS.
- Undiagnosed supraventricular arrhythmia.
- Ungrounded recording equipment affected by a nearby air-conditioner.
- How are the electrical artifacts and the respiratory events related?
- Apneas result in an increased cardiac preload and myocardial fiber stretch causing fine electrical discharges.
- The VNS activations cause spasm in the upper airway muscles resulting in obstructive apneas.
- During supraventricular arrhythmias, decreased cardiac output results in adverse respiratory events.
- The noise from the air-conditioner lowers the arousal threshold causing sleep instability and precipitates respiratory events.
Answers:
1. What is the cause of the elecrocardiogram artifacts?
B. Electrical activations of the implanted VNS.
2. How are the electrical artifacts and the respiratory events related?
B. The VNS activations cause spasm in the upper airway muscles resulting in obstructive apneas
Discussion:
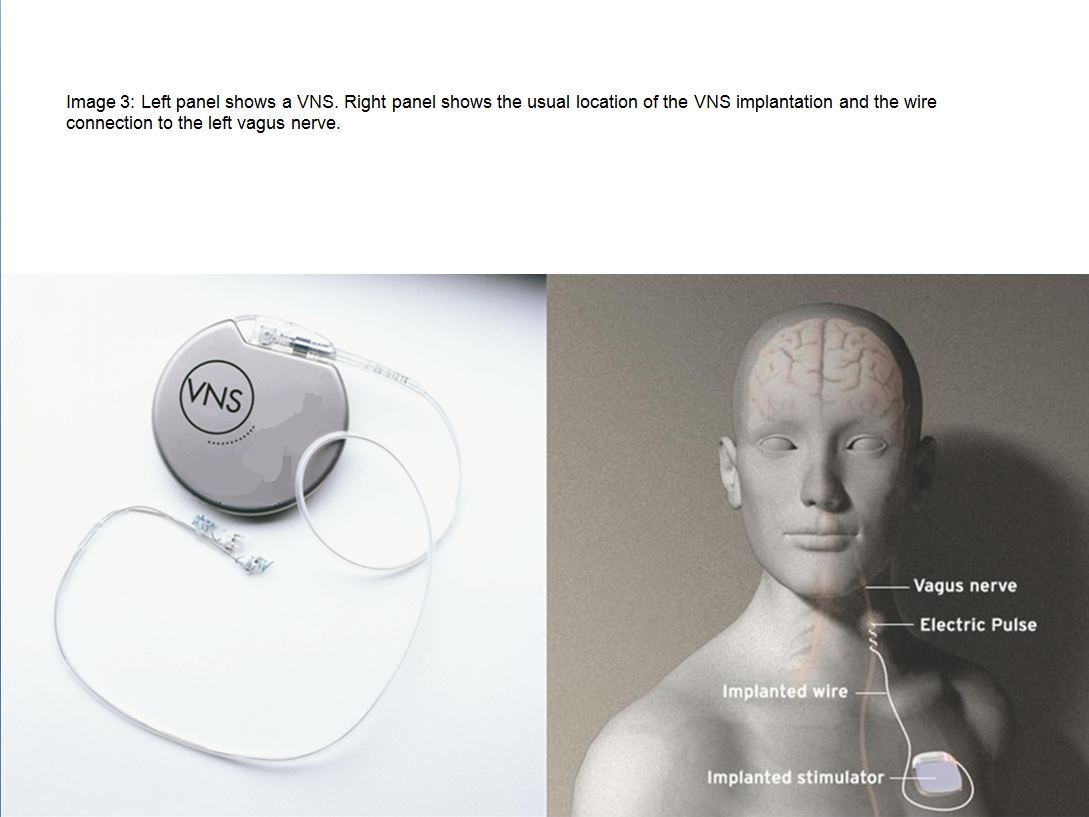
The patient has an implanted VNS to treat uncontrolled seizures. A VNS is usually implanted in the same area as a cardiac pacemaker, which explains the findings on this patient’s physical examination.
In 1997, the FDA approved the use of VNS (in patients 12 years of age or older) as an adjunctive seizure therapy. A VNS may also be used in the treatment of depression in select populations. The mechanism of action of vagal nerve stimulation in controlling seizures is unknown; however, electrical stimulation of the vagal nerve activates brainstem nuclei such as the nucleus solitarius. This action has been proposed as a mechanism for reduction of seizure frequency in humans. In some patients, activation of a VNS at seizure onset may also help abort a seizure (1).
Of course, artificial stimulation of the vagal nerve is not without unintended consequences. Some of the side effects of VNS activation include episodic hoarseness, cough, paresthesia, and dyspnea (2). These side effects occur via the activation of the recurrent laryngeal nerve by the VNS. Although our patient had intermittent hoarseness, he managed to camouflage it in a cleaver way: when the VNS fired while the patient was in the middle of a conversation, he used the duration of the activation to clear his throat. This was also noted during the clinical interview.
One more reported side effect of VNS activations is sleep disordered breathing (3,4). The mechanism of our patient’s symptoms was confirmed via direct endoscopic observation of his upper airway during activation of the VNS. The musculature of the pharyngeal sphincter seemed to contract to a tight closure during the periods of VNS activations. Applying a magnet to the patient’s implanted VNS resulted in its deactivation and in the resolution of the patients metronomic apneas.
References:
- Lado FA, Moshé SL. How do seizures stop? Epilepsia. 2008 Oct;49(10):1651-64.
- Morris GL 3rd, Mueller WM. Long-term treatment with vagus nerve stimulation in patients with refractory epilepsy. Neurology. 1999 Nov 10;53(8):1731-5.
- Holmes MD, Chang M, Kapur V. Sleep apnea and excessive daytime somnolence induced by vagal nerve stimulation. Neurology. 2003 Oct 28;61(8):1126-9.
- Marzec M, Edwards J, Sagher O, Fromes G, Malow BA. Effects of vagus nerve stimulation on sleep-related breathing in epilepsy patients. Epilepsia. 2003 Jul;44(7):930-5.


