Contributed by Vidya Krishnan, MD MHS, Division of Pulmonary, Critical Care and Sleep Medicine, MetroHealth Medical Center, Cleveland, OH
A 48 year old man was referred to our sleep center for complaints of snoring, difficulty maintaining sleep, and excessive daytime sleepiness (although his Epworth Sleepiness Score was only 3). He underwent a diagnostic polysomnography, with the following findings:
Lights out to lights on: 9:45pm to 4:05am (patient awoke and requested study end)
Sleep latency: 52 minutes
Wake after sleep onset: 129.5 minutes
Sleep efficiency: 52.3 %
REM latency: 35 minutes
N1 8.0 minutes (4%)
N2 102.5 minutes (53%)
N3 53 minutes (24%)
R 35 minutes (19%)
A representative 60-second epoch from the first REM period of the night is shown.
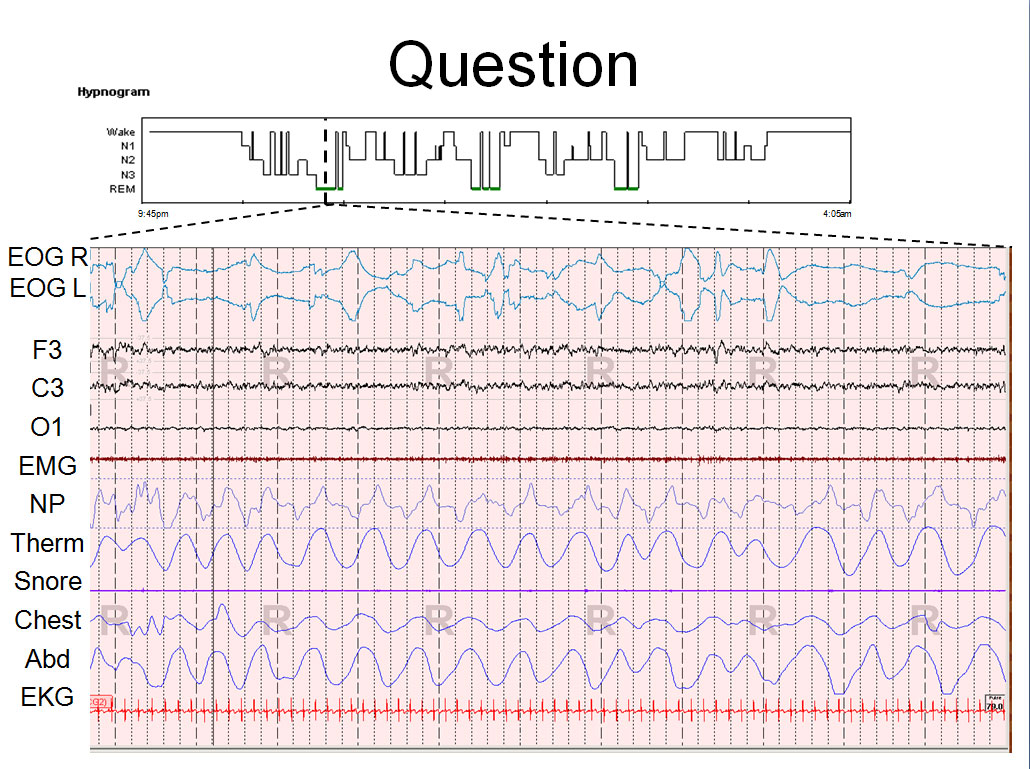
What is the most likely diagnosis suggested by the findings from the history and polysomnogram?
A. REM behavior disorderB. Major depressive episode
C. Narcolepsy
D. Use of anti-depressant medication
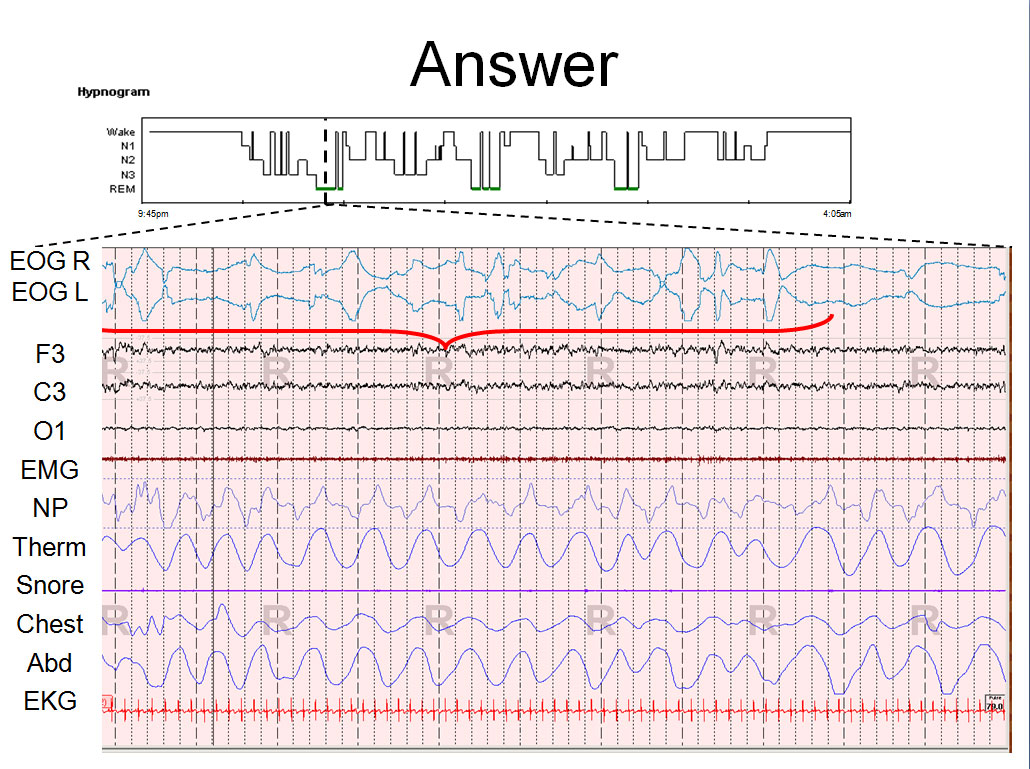
ANSWER:
B. Major depressive episode. Decreased REM latency, increased REM density, early morning awakening, increased wake after sleep onset and sleep continuity disturbances suggest a diagnosis of primary major depression. The high phasic activity during REM is highlighted, with over 15 rapid eye movements per minute of REM sleep in this fragment.
DISCUSSION:
Major depressive episode occurs when depressed mood or loss of interest occurs for at least two weeks, in addition to at least four other secondary symptoms. Sleep disturbances are common in depression, particularly early morning awakenings or frequent or prolonged awakenings at night. Polysomnographic abnormalities in major depression include 1) sleep continuity disturbances; 2) reduced N3 sleep stage; 3) decreased REM latency; 4) increased REM density; and 5) increased REM sleep early in the usual sleep period.[1] While no single PSG abnormality is particularly sensitive or specific, the more abnormalities found, the more likely the diagnosis. A high REM density (>12.56 REM’s/minute) is reported to have a sensitivity of 82% and specificity of 80% in one study.[2] The patient presented has #1, #3, #4 and #5, and was, on subsequent clinical evaluation, diagnosed with major depression.
REM density is a measure of the frequency of rapid eye movements during a REM sleep period. There is no consensus definition for REM density. Some studies use an index of number of rapid eye movements per minute of REM. Others have used minutes of REM with eye movements per total minutes of REM. While there is no definition of “normal REM density”, a generally accepted range is 4-5 rapid eye movements per minute of REM sleep.
REM density is known to increase over the course of a sleep episode, related to a decrease in sleep pressure.[3] An increase in sleep pressure (such as with sleep deprivation) has been associated with a decrease in REM density, which is often cited as a mechanism for sleep deprivation therapy for patients with major depression. Increased REM density has been described as a marker of severity of disease or poor prognostic factor in a number of psychiatric conditions, including relapse in recovering alcoholics, suicidal ideation in schizophrenic patients, and poor response to partial sleep deprivation and psychotherapy in patients with depression.[4]
Narcolepsy is another condition associated with decreased REM latency and increased REM density. However, there are a few reasons to suggest the alternate diagnosis in this vignette. There are no history elements given to suggest narcolepsy, such as cataplexy, hypnogogic or hypnopompic hallucinations, or sleep paralysis (although the history is admittedly brief). Excessive daytime sleepiness is reported by the patient, but subjective sleep propensity, as reflected by the Epworth Sleepiness Score (ESS), is only 3. The sensitivity and specificity of an ESS > 10 for the diagnosis of narcolepsy is 93.5% and 100%, respectively.[5] A comparison of REM sleep in narcoleptic patients vs. depressed patients was studied by Pollmacher and colleagues.[6] They reported narcolepsy patients had REM latency of <1 or >60 minutes, whereas depressed patients had REM latency 1-60 minutes. Narcolepsy patients with short sleep latency also had longer total sleep time, greater sleep efficiency, reduced amounts of wakefulness, and increased amounts of slow-wave sleep. Only the increased slow wave sleep was seen in the presented patient, also suggesting the diagnosis of depression over narcolepsy.
REFERENCES:
[1] American Academy of Sleep Medicine. The International Classification of Sleep Disorders, Second Edition. AASM, Westchester IL. 2005.
[2] King D, Akiskal HS, Lemmi H, Wilson W, Belluomini J, Yerevanian BI. REM Density in the Differential Diagnosis of Psychiatric From Medical-Neurologic Disorders: A Replication. Psychiatry Research. 1981; 5: 267-276.
[3] Khalsa SB, Conroy DA, Duffy JF, Czeisler CA, Dijk DJ. Sleep- and circadian-dependent modulation of REM density. J Sleep Res. 2002 Mar;11(1):53-9.
[4] Clark C, Dupont R, Golshan S, Gillin JC, Rapaport MH, Kelsoe JR. Preliminary evidence of an association between increased REM density and poor antidepressant response to partial sleep deprivation. J Affect Disord. 2000 Jul;59(1):77-83.
[5] Johns MW. Sensitivity and specificity of the multiple sleep latency test (MSLT), the maintenance of wakefulness test and the Epworth sleepiness scale: Failure of the MSLT as a gold standard. J Sleep Res. 2000; 9:5-11.
[6] Pollmächer T, Mullington J, Lauer CJ. REM sleep disinhibition at sleep onset: a comparison between narcolepsy and depression. Biol Psychiatry. 1997 Oct 15;42(8):713-20.


