Contributed by Tauseef Afaq, MD (Fellow, Sleep Medicine), Aneesa Das, MD (Assistant Professor, Sleep Medicine), Department of Internal Medicine, Division of Pulmonary, Allergy, Critical Care & Sleep Medicine, The Ohio State University, Columbus, Ohio
An 86 year old woman with a history of hypertension and hyperlipidemia is being evaluated by a neurologist for progressive cognitive and behavioral decline. Her recent neuropsychiatric and extended mental status examination is consistent with Alzheimer’s disease and she is started on memantine and galantamine. She is subsequently referred to sleep clinic for evaluation of daytime sleepiness, snoring and witnessed apneas. She goes to bed around midnight and gets up by 8 am. She denies excessive movements or arousals during sleep. Her physical exam reveals a BMI of 30.7 and mallampati score of 3. Her gross motor exam is with in normal limits. She underwent overnight polysomnography. Her sleep efficiency is 70% and her over-all AHI is 21.1 with oxygen nadir 71%.
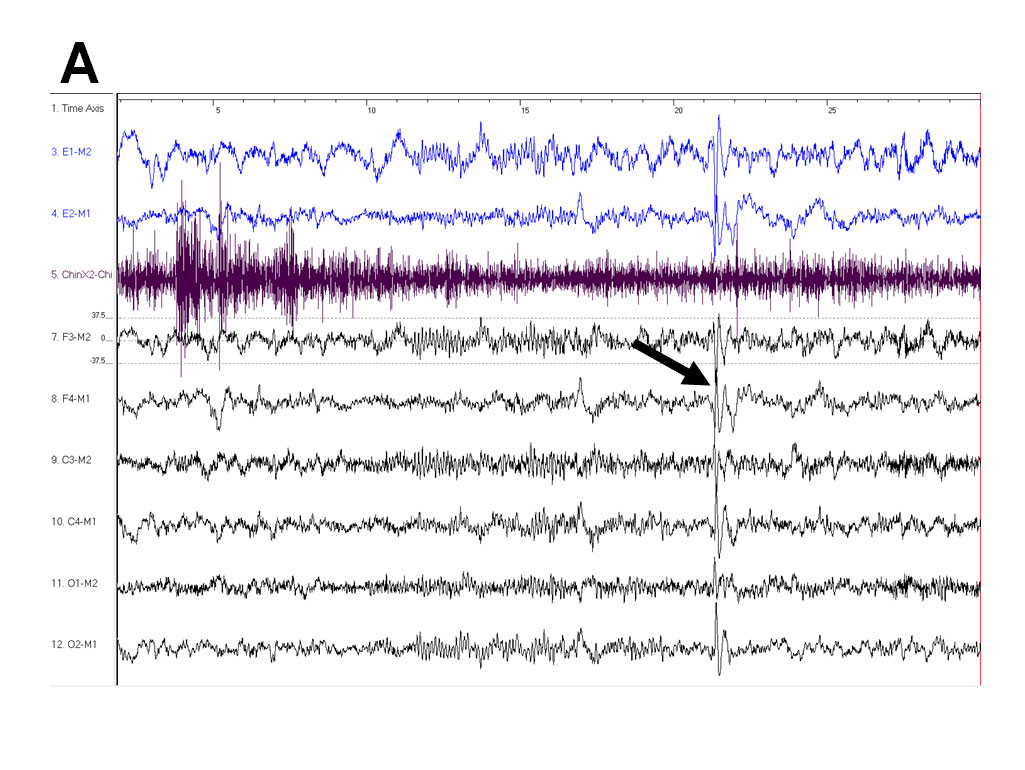
QUESTION 1: What does Epoch (A) show in terms of EEG activity at the arrow?
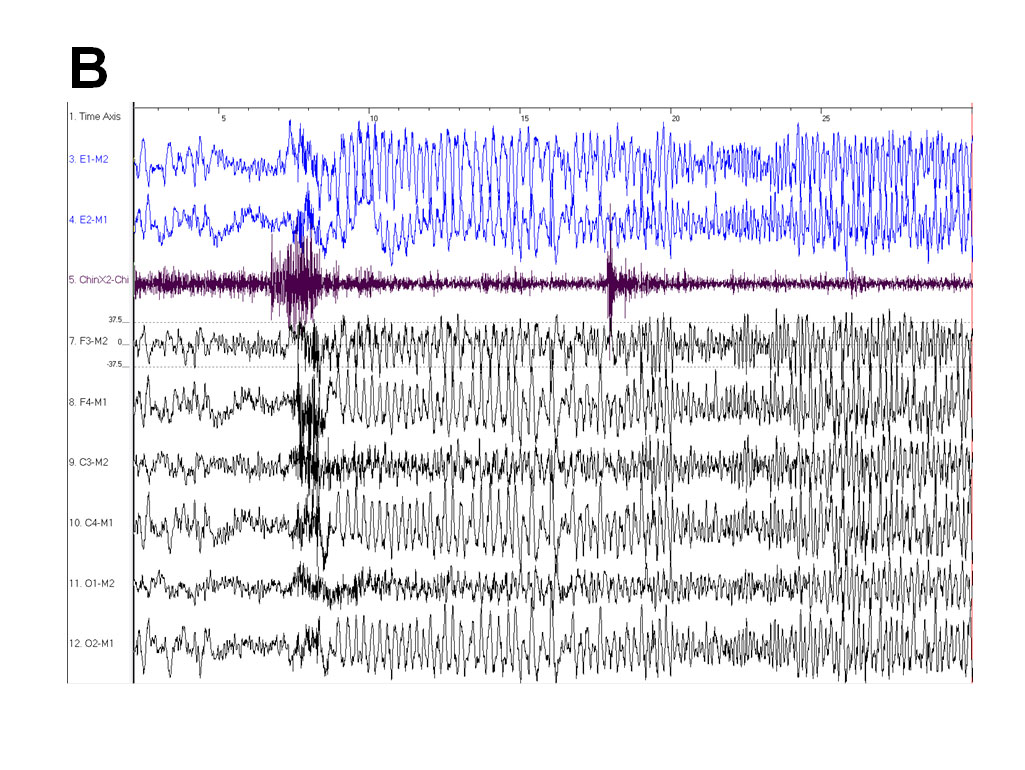
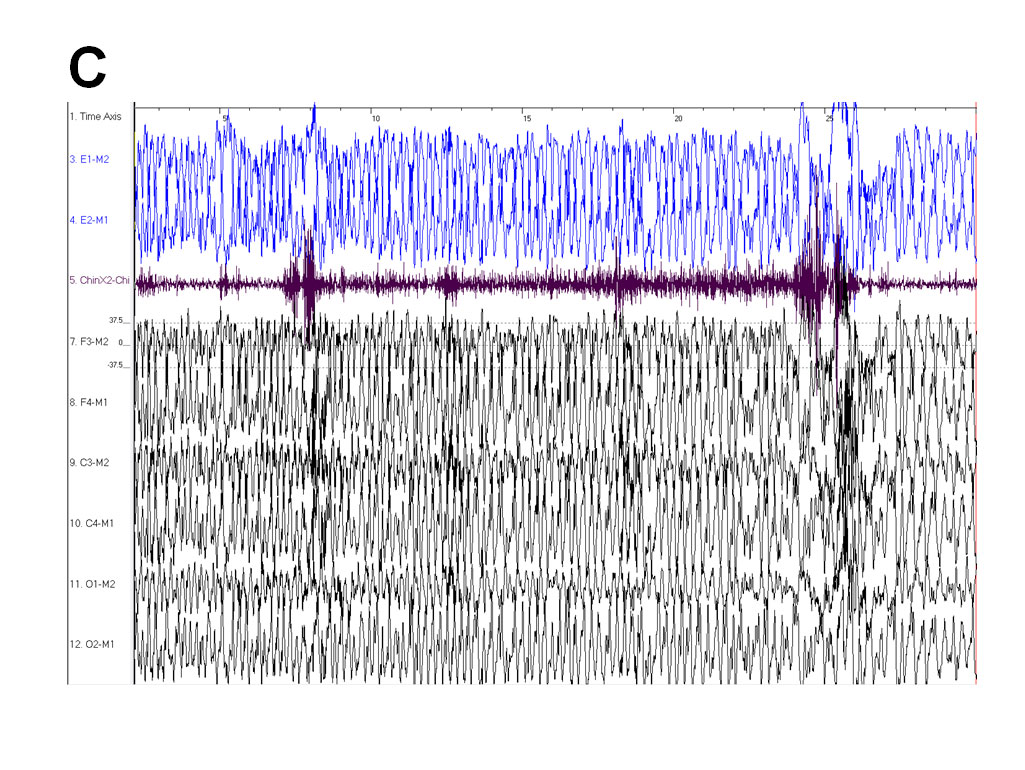
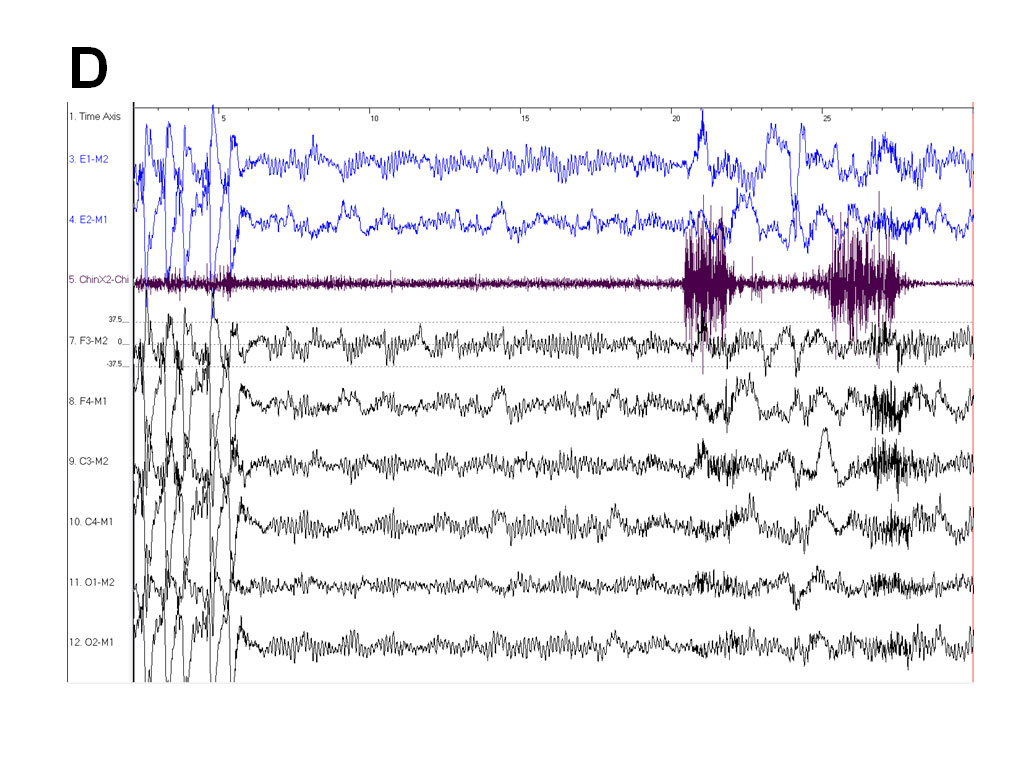
QUESTION 2: What do Epochs (B to D) represent in terms of EEG activity?
QUESTION 3: What in her history might be associated with this finding?
IMAGES:
ANSWER:
Answer 1: Interictal epileptiform discharge.
Answer 2: Subclinical ictal epileptiform activity.
Answer 3: Obstructive sleep apnea, Alzheimer’s Dementia, and Medications.
DISCUSSION:
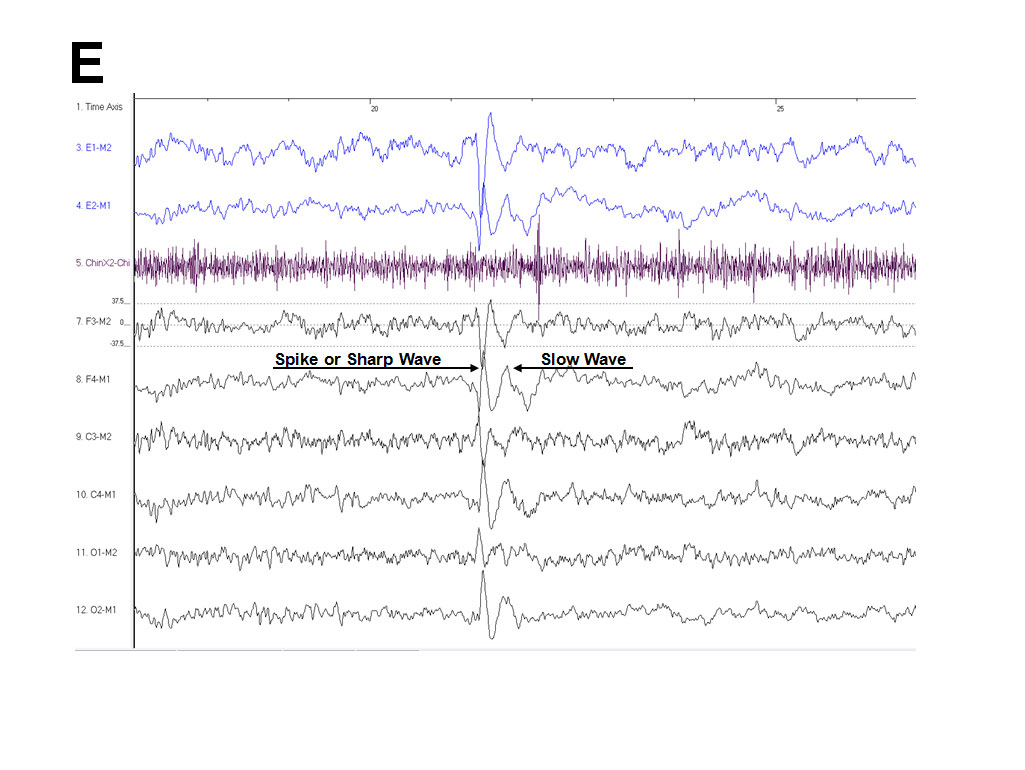
Interictal epileptiform discharges are brief epileptiform activities that occur without behavioral changes or impairment of consciousness. They begin with a fast component (spike or sharp-wave) followed by a slow-wave component (see Epoch A and E). They are usually brief in duration, typically lasting less than one second and almost always exceed the amplitude of surrounding background activity. In our patient we started noticing these discharges as shown in Epoch A. While interictal epileptiform discharges are asymmetric with two distinct components, non-epileptiform transients are typically symmetric thus helping to distinguish the two.
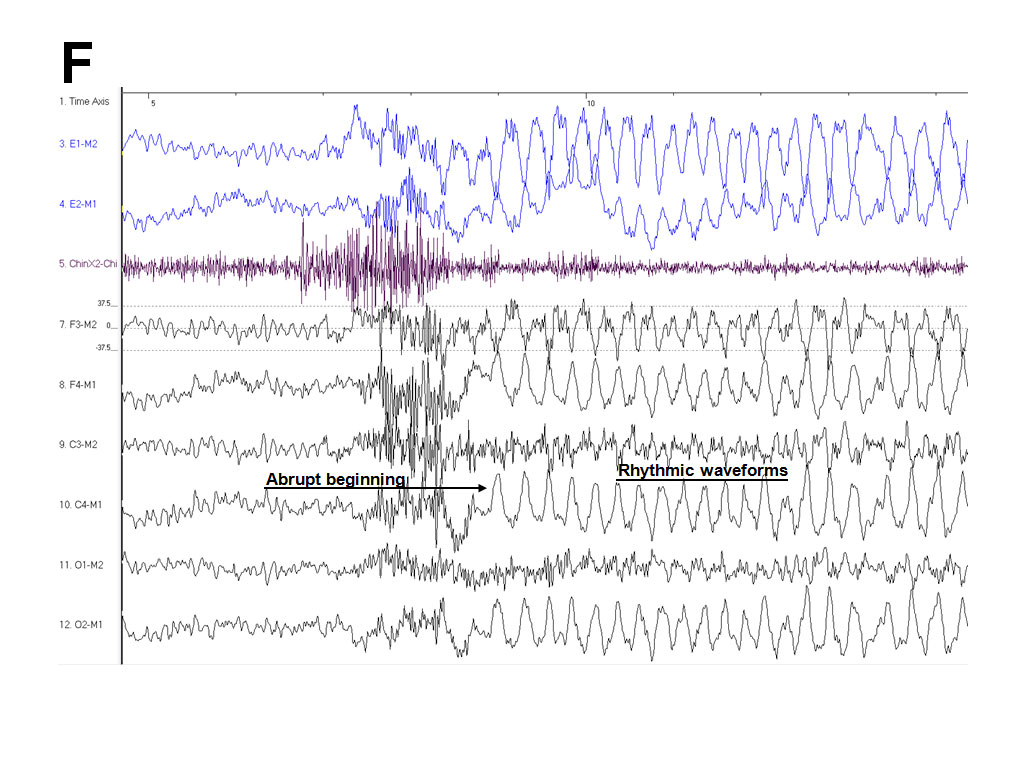
Localized ictal epileptiform activity is also known as electrographic seizure activity. It usually persists for more than several seconds, begins abruptly (see Epoch B and F), and consists of repetitive and rhythmic waveforms that tend to vary in form, frequency and topography through out the seizure (see Epoch B-D and F). Epoch F shows ictal epileptiform activity at standard EEG rates of 30mm/sec. In our patient, tonic-clonic activity was not noted on video monitoring, although there was increase in chin EMG tone (see Epoch C). Ictal EEG patterns that occur in the absence of clinical seizure manifestations are referred to as subclinical ictal or subclinical electrographic seizure activity. Our patient was in NREM sleep during these discharges. Seizures are more common in NREM sleep than in wakefulness or REM sleep but are often subclinical (1). Our patient was subsequently referred for a formal electroencephalogram which confirmed subclinical epileptic activity.
Alzheimer’s disease is a risk factor for the development of late-onset unprovoked epileptic seizures (2). Epilepsy affects about 3.6% of patients with Alzheimer’s dementia (3). Young age, African American ethnicity, more severe dementia and focal epileptiform findings on EEG are associated with increased likelihood of unprovoked seizures in patients with Alzheimer’s disease(4).
Obstructive sleep apnea has been shown to be associated with seizure exacerbation in older adults with epilepsy, and its treatment may be important for improving seizure control in this population (5). Malow et al found that there is an increased prevalence of obstructive sleep apnea in medically refractory epilepsy patients suggesting a possible association between the two (6). Our patient was found to have moderate obstructive sleep apnea and she was started on continuous positive airway pressure therapy.
Alzheimer’s medications have been associated with seizures as well. There is a case report of Memantine as a potential cause of seizure in Alzheimer’s disease patient (7). Galantamine appears to be safe and tolerable in patients with epilepsy.
Obstructive sleep apnea and Alzheimer’s disease share many common risk factors including increasing age. Untreated obstructive sleep apnea itself can have deleterious effects on cognition and daytime functioning, and may exacerbate the primary cognitive and functional deficits associated with Alzheimer’s disease. It has been reported that sustained and long term CPAP treatment for patients with Alzheimer’s disease and obstructive sleep apnea may result in lasting improvements in sleep and mood as well as a slowing of cognitive deterioration (8).
REFERENCES:
1. Minecan D, Natarajan A, Marzec M, Malow B. Relationship of epileptic seizures to sleep stage and sleep depth. Sleep. 2002 Dec;25(8):899-904.
2. Romanelli MF, Morris JC, Ashkin K, Coben LA. Advanced Alzheimer's disease is a risk factor for late-onset seizures. Arch Neurol 1990 Aug;47(8):847-50.
3. Rao SC, Dove G, Cascino GD, Petersen RC. Recurrent seizures in patients with dementia: frequency, seizure types, and treatment outcome. Epilepsy Behav 2009 Jan;14(1):118-20.
4. Amatniek JC, Hauser WA, DelCastillo-Castaneda C, Jacobs DM, Marder K, Bell K, Albert M, Brandt J, Stern Y. Incidence and predictors of seizures in patients with Alzheimer's disease. Epilepsia 2006 May;47(5):867-72.
5. Chihorek AM, Abou-Khalil B, Malow BA. Obstructive sleep apnea is associated with seizure occurrence in older adults with epilepsy. Neurology 2007 Nov 6;69(19):1823-7.
6. Malow BA, Levy K, Maturen K, Bowes R. Obstructive sleep apnea is common in medically refractory epilepsy patients. Neurology 2000 Oct;55(7):1002-7.
7. Peltz G, Pacific DM, Noviasky JA, Shatla A, Mehalic T. Seizures associated with memantine use. Am J Health Syst Pharm 2005 Feb 15;62(4):420-1.
8. Cooke JR, Ayalon L, Palmer BW, Loredo JS, Corey-Bloom J, Natarajan L, Liu L, Ancoli-Israel S. Sustained use of CPAP slows deterioration of cognition, sleep, and mood in patients with Alzheimer's disease and obstructive sleep apnea: a preliminary study. J Clin Sleep Med 2009 Aug 15;5(4):305-9.


