Contributed by Robert M. Jones, MD, Joanne Coleman, NP MSN, Eric M. Davis, MD Division of pulmonary and critical care, Department of Medicine, University of Virginia, Charlottesville, VA, USA Corresponding Author: Eric M. Davis University of Virginia - Pulmonary and Critical Care Division, Dept of Medicine PO Box 800682 Charlottesville Virginia 22908-0682 United States Author Contributions: All authors contributed to the writing and preparation for the manuscript. Conflict of Interest: All authors report that they have no conflicts of interest or financial conflicts related to this manuscript. The views expressed in this article do not communicate an official position of the University of Virginia. Key Words: tension pneumocephalus. CPAP complications. VP shunt
Case Vignette
A 33 year old man presented with 3 weeks of worsening of his chronic headache. The headache was exacerbated in the upright position and associated with left foot weakness and numbness. He had a remarkable, yet remote, medical history of a motor vehicle collision (MVC) 14 years prior resulting in a closed head injury with a right occipital lobe hemorrhagic contusion and multiple craniofacial fractures involving both the orbital roof and sphenoid sinus. He required decompressive craniotomy that hospitalization. Two years later he sustained a second traumatic intracerebral hemorrhage after falling during a seizure. He required ventriculoperitoneal (VP) shunt placement for post-traumatic hydrocephalus.
In between these hospitalizations, the patient underwent investigation of excessive daytime sleepiness, that per the patient predated his MVC and may have been a contributing factor. His Epworth Sleepiness Scale was 18/24. He underwent polysomnography that revealed a total apnea hypopnea index (AHI) of 18 events/hour, an obstructive AHI of 17.8 events/hour and a central apnea index of < 0.2 events/hour. He subsequently underwent a continuous positive airway pressure (CPAP) titration study and was prescribed CPAP therapy at 9 cm H2O. During follow-up, the patient reported an improvement in his daytime sleepiness and download data from his CPAP unit suggested adherence at 90% of nights with a normal residual AHI.
Fourteen years after his MVC, 13 years after initiation of CPAP therapy, and 12 years after his VP shunt placement the patient presented with the aforementioned headache. His physical exam on this presentation was notable for mild mental slowing and 1+ out of 5+ strength in both plantar and dorsiflexion of his left lower extremity. Computed tomography (CT) of the head was performed (Figure 1).
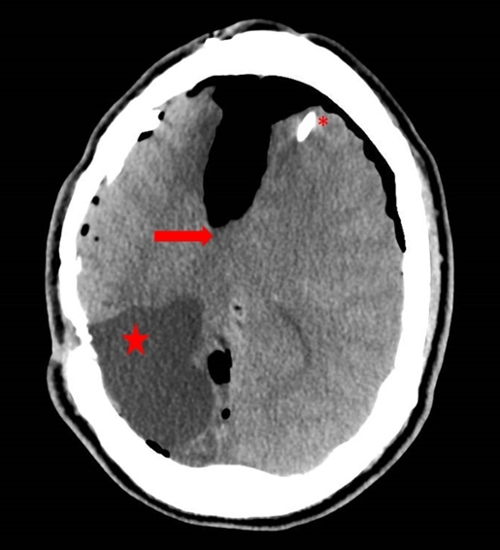
Figure 1: CT head showing acute changes associated with midline shift (arrow), ventriculo-peritoneal shunt (*), and encephalomalacia from prior right occipital hemorrhage (star).
Questions
- What potential complication of positive airway pressure (PAP) therapy is demonstrated in Figure 1?
- Which patients undergoing PAP therapy are at risk of developing pneumocephalus?
- How is tension pneumocephalus best managed?
Discussion
Pneumocephalus is defined as air within the intracranial vault. Tension pneumocephalus is present when air accumulation leads to increased intracranial pressure with neurological decline. Pneumocephalus most commonly occurs in the setting of craniofacial trauma and neurosurgical or otolaryngological procedures. Infiltrating tumors, CNS infections with gas forming organisms, barotrauma, and application of Valsalva maneuver are also reported etiologies (1, 2).
Various mechanisms have been proposed for the development of pneumocephalus. A ball valve effect occurring with a CSF leak is thought to be one mechanism, whereby air can enter through a CSF leak but as intracranial pressure increases, the defect closes and the air is trapped. It is plausible that this effect is exacerbated by Valsalva maneuvers (sneezing and coughing) and potentially PAP therapy. A second possible mechanism is when CSF leak creates negative intracranial pressure and air enters the CSF in order to balance the pressure. Pneumocephalus can also occur due to gas forming organisms in CNS infections (1).
Pneumocephalus in association with PAP therapy is a rare but potentially life-threatening complication. It is most commonly noted in the setting of recent craniofacial trauma or neurosurgical procedures (3). Unlike in our case, the cases associated with craniofacial trauma are typically associated with pre-hospital PAP via bag-valve-mask ventilation or preoperative PAP therapy (4). There are reports of pneumocephalus occurring spontaneously with PAP therapy in which atraumatic CSF leaks were found (5, 6). The use of PAP therapy in the presence of ventriculoperitoneal shunts has also been associated with pneumocephalus at various intervals from shunt placement, up to 3 years, far shorter of a timeframe than our case (7). Our patient was free from potential dural insults (MVC and VP shunt placement) for greater than 10 years suggesting that the pneumocephalus potentially resulted from PAP therapy in this high risk patient.
Pneumocephalus can present with headaches, dizziness, cranial nerve palsies, cerebrospinal fluid rhinorrhea, decreased levels of consciousness, and seizures. There are descriptions of "splashing" or "gurgling" sensations. In our case the predominant findings were the positional headache and the focal weakness (8). Head CT is more sensitive than the skull radiograph in detecting intracranial air and is the diagnostic modality of choice.
Management of pneumocephalus depends on the presence of neurologic deficits. Asymptomatic pneumocephalus can be managed conservatively whereas tension pneumocephalus is considered a neurosurgical emergency. Prompt decompression of intracranial air is required and surgical treatment options include drilling of burr holes, needle aspiration, ventriculostomy and craniotomy. In the presence of VP shunts, increasing the valve opening pressure is typically performed. Identification and correction of any potential CSF leaks should be performed. The risks and benefits of future PAP therapy should be considered on a case to case basis dependent on the likely etiology.
Answers
-
What potential complication of PAP therapy is demonstrated in Figure 1?
Pneumocephalus is a rare but potential complication of PAP therapy. -
Which patients undergoing PAP therapy are at risk of developing pneumocephalus?
Patients with a potential dural defect are at risk for developing pneumocephalus, even if such a dural defect occurred in the remote past. -
How is tension pneumocephalus best managed?
Tension pneumocephalus is a potential neurosurgical emergency and indication for cranial decompression.
Follow-Up
Following his acute presentation, our patient underwent emergent decompression via adjustment of his VP shunt settings followed by needle decompression of his tension pneumocephalus. He underwent neuroimaging without any clear evidence of CSF leak. At a follow up visit he had resolution of his headaches and focal neurologic deficits. Given inability to find a repairable defect and his now mild obstructive apnea it was felt the risks of ongoing PAP therapy outweighed any benefits.
This case highlights the need to be mindful of the risk of pneumocephalus with PAP therapy in patients with potential dural defects, regardless of the time since insult.
References
-
Dabdoub CB, Salas G, Silveira Edo N, Dabdoub CF. Review of the management of pneumocephalus. Surg Neurol Int. 2015 Sep 29; 6: 155-7806.166195. eCollection 2015. PMCID: PMC4596054.
-
Markham JW. The clinical features of pneumocephalus based upon a survey of 284 cases with report of 11 additional cases. Acta Neurochir (Wien). 1967; 16(1): 1-78.
-
Klopfenstein CE, Forster A, Suter PM. Pneumocephalus. A complication of continuous positive airway pressure after trauma. Chest. 1980 Oct; 78(4): 656-657.
-
Rathore AS, Satyarthee GD, Mahapatra AK. Post-traumatic tension pneumocephalus: Series of four patients and review of the literature. Turk Neurosurg. 2016; 26(2): 302-305.
-
Bernstein AL, Cassidy J, Duchynski R, Eisenberg SS. Atypical headache after prolonged treatment with nasal continuous positive airway pressure. Headache. 2005 May; 45(5): 609-611.
-
Jarjour NN, Wilson P. Pneumocephalus associated with nasal continuous positive airway pressure in a patient with sleep apnea syndrome. Chest. 1989 Dec; 96(6): 1425-1426.
-
Chee BN, Abdul Jalil MF, Bulluss KJ. Spontaneous pneumocephalus from nasal continuous positive airway pressure in a patient with ventriculo-peritoneal shunt. J Clin Neurosci. 2016 Aug 16.
-
El-Sayed I, Saleh H, McDermott M. Neurosurgical complications. In: Eisele D, Smith R, editors. Complications in Head and Neck Surgery. 2nd ed. London: Mosby; 2009. p. 119-119-132.


