Contributed by Lourdes M. DelRosso, MD, FAASM (1); Michelle Y. Sobremonte-King, MD, FAAP, FAASM (2); Christopher M. Cielo, D.O (1), Romy Hoque, MD, FAASM (3) (1) The Children’s Hospital of Philadelphia, Division of Pulmonary Medicine Philadelphia, PA (2) Children's Hospital Colorado Breathing Institute, Aurora, CO (3) Emory Sleep Center, Department of Neurology, Atlanta, GA Corresponding Author: Lourdes M. DelRosso, MD, FAASM Email: lourdesdelrosso@me.com Phone 267-559-4515 Authors’ Contributions: Dr. DelRosso wrote the case, table, chose images and the overall structure of the discussion Dr. Sobremonte-King contributed with the discussion of mechanism of central apnea Dr. Hoque contributed with the mechanism and treatment options. Dr. Cielo contributed with follow up data and figures. Conflicts of Interest: The authors do not have any support or conflict of interest to report Short Title: Treatment emergent central apnea in a child
Case Vignette
A 7-year-old girl with trisomy 21 was brought to medical attention because of persistent snoring after an adenotonsillectomy. She had hypothyroidism and gastroesophageal reflux disease. Her medications included levothyroxine, nasal fluticasone and ranitidine. Physical examination revealed height and weight in the 45th percentile (Trisomy 21 chart), features of trisomy 21, modified Mallampati III and absent tonsils.
A polysomnogram (PSG) showed obstructive sleep apnea with hypoventilation, an obstructive apnea-hyponea index (AHI) of 6.2 events per hour, a central AHI of 3 events per hour, an oxygen saturation nadir of 89%, and hypoventilation with an end-tidal pCO2 of 50-51 Torr for 78% of total sleep time.
She was initiated on nasal fluticasone and bilevel positive airway pressure (BPAP) 8/4 cm H20 set in the spontaneous mode. She had poor adherence to BPAP, waking several times during the night pulling at her mask.
Given difficulties tolerating BPAP, the patient underwent a PAP titration study. The results are shown in Table 1 and the hypnogram is depicted in Figure 1. Total sleep time was 501 minutes. The arousal index was elevated at 25 events per hour. An optimal PAP could not be determined on the night of the study and on BPAP 8/4 cm H20 a new pattern of respiration shown in Figure 2 was seen.
| PAP pressure (cmH2O) | Time at pressure (min) | REM time (min) | Obstructive AHI (events/hr) | Central AHI (events/hr) | Nadir Saturation (%) | Mean ptcCO2 |
|---|---|---|---|---|---|---|
| 8/4 | 181 | 15 | 6 | 24.5 | 92 | 51 |
| 4 | 90 | 15 | 4 | 12 | 94 | 51 |
| Off | 230 | 79 | 4 | 5 | 93 | 49 |
ptcCO2= transcutaneous CO2
Table 1 Positive airway pressure titration results.
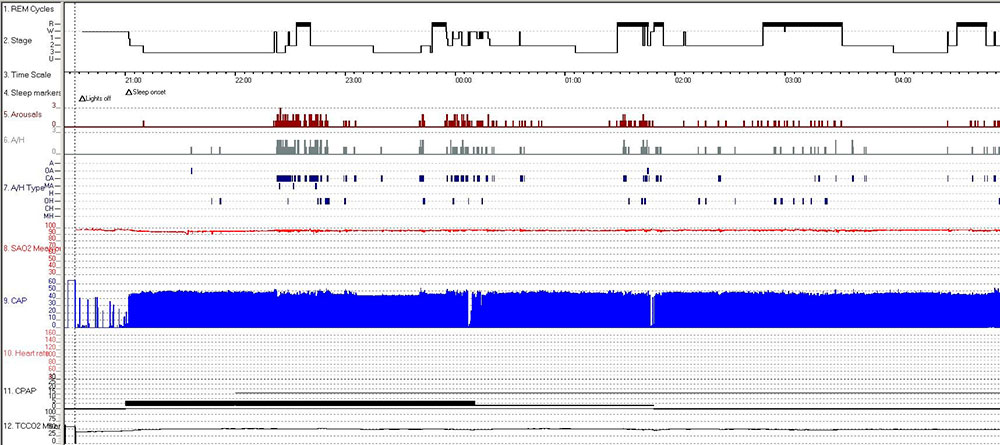
Figure 1: Hypnogram. REM (rapid eye movement), Stage R (REM), W (Wake), A/H type (apnea/hypopnea, A (apnea), OA (obstructive apnea), CA (central apnea), MA (mixed apnea), H (hypopnea), OH (obstructive hypopnea), CH (central hypopnea), MH (mixed hypopnea); SAO2 (oxyhemoglobin saturation), CAP (capnography), CPAP (continuous positive airway pressure), TCCO2 (transcutaneous CO2)
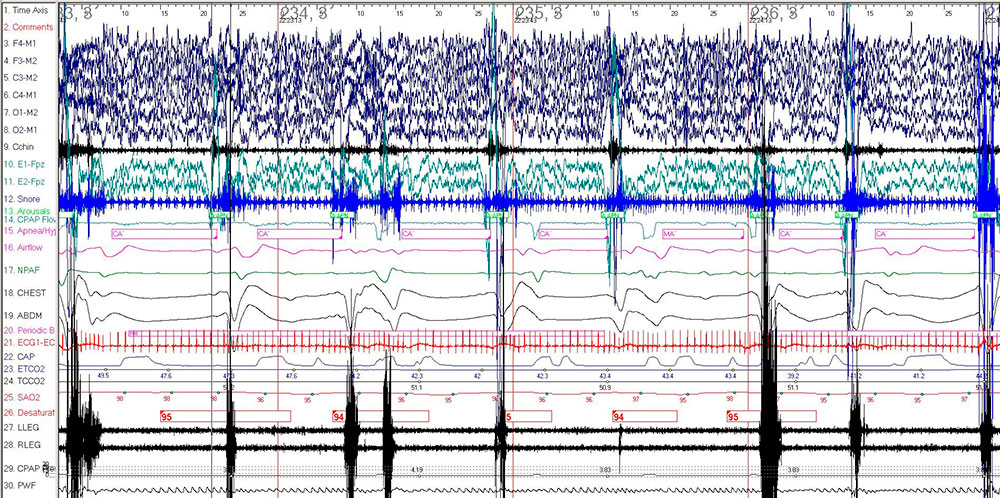
Figure 2: 2-minute epoch on BPAP 8/4 cm H2O. Electroencephalogram leads (F4-M1, F3-M2, C3-M2, C4-M1, O1-M2, O2-M1); Electromyogram leads (Cchin, LLEG, RLEG), Ocular leads (E1-M2, E2-M1), Respiratory sensors (NPAF, Airflow), EKG leads (ECG1, ECG2), CAP (capnography), SAO2 (oxyhemoglobin saturation), PWF (pulse wave form).
Questions
- What diagnosis is suggested based on the results of Table 1?
- What are the proposed mechanisms producing the breathing pattern shown in Figure 2?
- What is the best treatment option?
Discussion
Figure 2 depicts central apneas on positive airway pressure. The development of central apnea in OSA patients during administration of PAP has been described in adults and referred to as treatment-emergent central sleep apnea or complex sleep apnea.
The International Classification of Sleep Disorders 3rd edition (ICSD-3) diagnostic criteria for treatment-emergent central sleep apnea include: i) diagnosis of OSA (obstructive AHI >5 per hour); ii) significant resolution of obstructive events with emergence or persistence of central events (central AHI > 5, number of central events > 50% of the total respiratory events) using PAP; and iii) absence of another better explanation for the central sleep apnea (CSA). Treatment emergent CSA has been reported in adults with PAP therapy, oral appliance therapy, nasal expiratory positive airway pressure, nasal surgery and maxillo-mandibular advancement.
Treatment-emergent central sleep apnea has not been clearly defined in children, hence the possible persistence of obstructive events in our patient compared to the usual resolution of obstructive events described in adult patients. A diagnosis of treatment-emergent CSA does not exclude a diagnosis of OSA. Patients with trisomy 21 are at increased risk of both central and obstructive apnea with CSAs frequently preceded by sighs. It is unknown whether the central apneas seen in our patient could have been explained by trisomy 21 but the significant increase in central events with PAP suggested treatment-emergent CSA. Similarly arterial blood gas data and pulmonary function testing would have been helpful in our patient to exclude other causes for CSA and hypoventilation.
The mechanisms by which PAP have been postulated to induce central apnea are complex and remain incompletely understood. Central apneas can occur due to increased arousals and sleep state instability, possibly from PAP intolerance. The resulting ventilatory response to arousals can lower the PaCO2 below the apneic threshold, leading to central apneas.The arousal index was elevated for our patient on the titration study. The relief of upper airway obstruction with PAP further improves CO2 excretion and can also lead to emergence of central apneas. Similarly, mask leaks can result in lowered PaCO2 levels by washing out anatomical dead-space, and central apneas can again occur if the resulting PaCO2 level falls below the apneic threshold.
Overtitration of PAP can lead to excessive increase in lung volume and transpulmonary pressure, stimulating stretch receptors located in the airway smooth muscles. This induces several physiologic responses, one of them being the inhibition of inspiration, which is known as the Hering Breuer reflex. The mechanisms described are taken in the context of the "loop gain" theory, which is the ventilatory response to a given change in PaCO2 or PaO2 levels. This can vary between individuals. Patients with high loop gain have increased chemosensitivity to changes in PaCO2 or PaO2, thereby over ventilating and lowering the PaCO2 below the apneic threshold. As such, a high loop gain has been proposed as one mechanism for persistent central apneas on PAP.
Therapeutic options for treatment-emergent sleep apnea are not well defined in either adults or children. Resolution of central events has been described in most patients with ongoing CPAP therapy, and as a rule, the lowest PAP pressure required to manage the obstructive apnea and minimize over ventilation is recommended. Additional research is needed before more definitive recommendations can be made regarding management of treatment-emergent CSA. In children, even greater uncertainties exist.
Answers
-
What diagnosis is suggested based on the results of Table 1?
Treatment-emergent central sleep apnea -
What are the proposed mechanisms producing the breathing pattern shown in Figure 2?
Lowering of the PaCO2 below the apneic threshold caused by increased arousals and relief of upper airway obstruction, activation of pulmonary stretch receptors, and high loop gain have been proposed as mechanisms for treatment-emergent CSA -
What is the best treatment option?
The optimal treatment for treatment-emergent CSA is unknown but PAP using the lowest pressure needed to control the obstructive events is suggested.
Follow-Up
Due to the mild severity of her sleep disordered breathing and worsened sleep quality using PAP therapy, PAP was discontinued. The patient continued management with nasal steroids and close observation. Otolaryngology consultation was recommended to evaluate for adenoidal regrowth or enlarged lingual tonsils.
References
- Avidan AY, Guilleminault C, Robinson A. The development of central sleep apnea with an oral appliance. Sleep Med. 2006;7(2):187-191.
- Chopra A, Das P, Ramar K, Staats B, St Louis EK. Complex sleep apnea associated with use of nasal expiratory positive airway (nEPAP) device. J Clin Sleep Med. 2014;10(5):577-579.
- Corcoran S, Mysliwiec V, Niven AS, Fallah D. Development of central sleep apnea after maxillofacial surgery for obstructive sleep apnea. J Clin Sleep Med. 2009;5(2):151-153.
- Goldstein C, Kuzniar TJ. The emergence of central sleep apnea after surgical relief of nasal obstruction in obstructive sleep apnea. J Clin Sleep Med. 2012;8(3):321-322.
- Ferri R, Curzi-Dascalova L, Del Gracco S, Elia M, Musumeci SA, Stefanini MC. Respiratory patterns during sleep in Down's syndrome:importance of central apnoeas. J Sleep Res. 1997;6(2):134-141.
- Wang J, Wang Y, Feng J, Chen BY, Cao J. Complex sleep apnea syndrome. Patient Prefer Adherence. 2013;7:633-641.
- Stanchina M, Robinson K, Corrao W, Donat W, Sands S, Malhotra A. Clinical Use of Loop Gain Measures to Determine Continuous Positive Airway Pressure Efficacy in Patients with Complex Sleep Apnea. A Pilot Study. Ann Am Thorac Soc. 2015;12(9):1351-1357.


