Contributed by Sameh S. Morkous1, O’Dene H. Lewis1, Dennis Auckley2 1Department of Pulmonary, Critical Care and Sleep Medicine, University Hospitals Case Medical Center, Cleveland, OH, USA 2Division of Pulmonary, Critical Care and Sleep Medicine, MetroHealth Medical Center, Case Western Reserve University, Cleveland, OH, USA Corresponding Author: Sameh S. Morkous University hospital - Pulmonary and Sleep medicine 11100 Euclid avenue Cleveland Ohio 44106 United States T: 216-983-0871 F: 216-844-2187
In Brief
A 9-year-old male presented to the sleep clinic for evaluation of abnormal behavior during sleep. The referring physician was concerned about a possible underlying sleep disorder versus a neurological problem. Polysomnography provided the answer.
Case Vignette
A 9-year-old male presented with nonrestorative sleep and abnormal behaviors during sleep. There were no reports of snoring, witnessed apneas, sleep walking or sleep talking, but the parents reported episodes of thrashing in bed at night, since the age of 2. These spells typically occurred 45-60 minutes after the patient went to bed. The abnormal activity, described as whole body rocking, would last for up to 30 minutes. Then the child fell back asleep. There was no event recall and no report of tongue biting or bladder or bowel incontinence. He was otherwise well except for generalized anxiety. His only medication was a daily multivitamin. The child did not use caffeinated beverages.
His body mass index was 15.7 kg/m2 (35th percentile BMI-for-age). Examination
revealed a Mallampati score of 2 and 1-2+ tonsil size. The remainder of the physical examination was normal.
A nocturnal polysomnogram was performed. Total sleep time was 350 minutes, sleep
latency 51 minutes, sleep efficiency 76.6%, and wake after sleep onset time was 55.5 minutes. The apnea-hypopnea index was 1.9 events per hour, and the arousal index was 6.9 per hour.
The lowest oxygen saturation was 92% and the mean EtCO2 was 31 mmHg. The periodic limb movement index was 0.9 events per hour. There were 46 episodes of whole body rocking behavior during transitions to sleep with the longest episode being 187 seconds. Three representative 30 seconds epochs from the patient’s polysomnogram are shown in the Figures
Questions
- What is the most likely diagnosis?
- What is the most appropriate next step in the management of this patient?
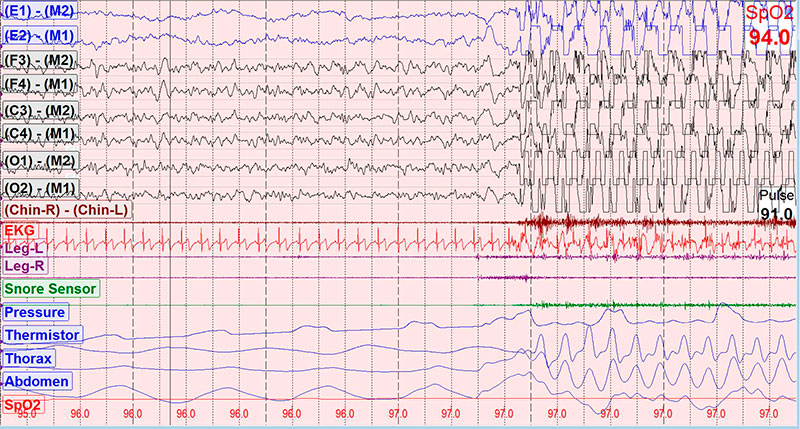
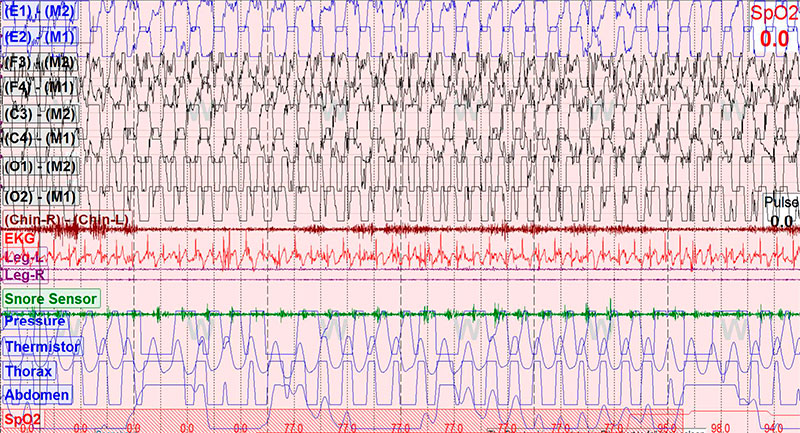
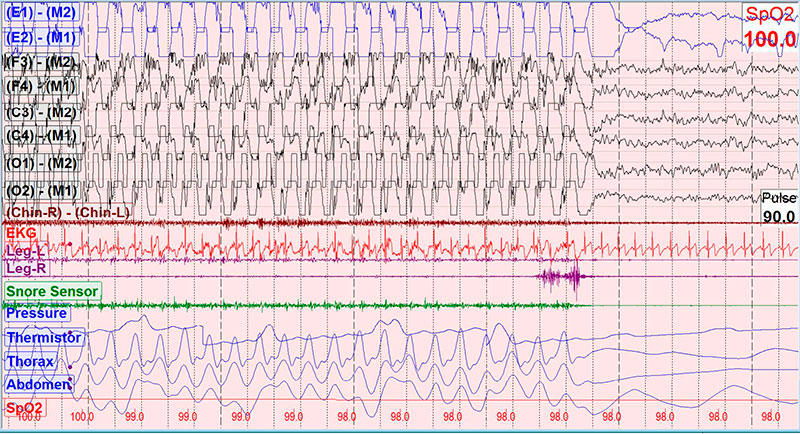
Figure Legend
30-second epochs recorded during wakefulness in the supine position. Panels A, B, and C show the onset, continuation, and termination of a typical event, respectively.
Discussion
The patient described in this report met the diagnostic criteria for rhythmic movement disorder. This condition is also sometimes referred to as body rocking, head banging, or head or body rolling.
According to the 3rd edition of the International Classification of Sleep Disorders the diagnosis of rhythmic movement disorder requires all of the following be met (1):
- The patient exhibits repetitive, stereotyped and rhythmic motor behaviors involving large muscle groups.
- The movements are predominantly sleep related, occurring near naps or bedtime, or when the patient appears drowsy or asleep.
- The behaviors result in a significant complaint characterized by at least one of the following:
- Interference with normal sleep;
- Significant impairment of daytime functioning;
- Self-inflicted body injury.
- The rhythmic movements are not better explained by another movement disorder or epilepsy.
"Significant clinical consequence" is what differentiates rhythmic movement disorder from sleep-related movements that are part of normal development (59% of 9-month-old infants exhibit some sleep related rhythmic movements, which decreases to 5% by 5 years old (2)).
Polysomnography (PSG) is often performed to verify the diagnosis and rule out other causes of the behavior. Characteristic findings include a minimum and maximum movement frequency of 0.5 and 2 Hz, respectively, a minimum of 4 rhythmic movements in a cluster and minimum amplitude on the electromyography (EMG) of a rhythmic burst twice the background EMG activity (3). Time synchronized video PSG is recommended to help make the diagnosis (4).
Rhythmic movements occur most often during N1 and N2 sleep, though they can occur with drowsiness (1). In the patient described here, almost all of the rhythmic movements occurred during wake-sleep transitions or N2 sleep, and were not associated with infrequent respiratory events.
The soothing effect of vestibular stimulation has been proposed as the reason infants and toddlers exhibit this behavior, possibly to promote development of the motor system. More recently, the inhibitory control system of the central motor pattern generator has been suggested to play a role in both pediatric and adult rhythmic movement disorder (5).
The differential diagnoses include repetitive movements restricted to small muscle groups (e.g. bruxism or rhythmic thumb sucking) and sleep related epilepsy. In this patient, the activity involved large muscle groups. Associated features of sleep-related seizures were absent and there was no epileptiform activity noted on the electroencephalogram (EEG). Also included in the differential diagnosis are the more common varieties of childhood parasomnias such as sleep terrors, sleep walking or confusional arousals. Secondary rhythmic movements have been reported in association with restless leg syndrome, obstructive sleep apnea, narcolepsy, REM behavioral disorder and attention deficit hyperactivity disorder (6).
This patient had mild obstructive sleep apnea, though this was not felt to be a contributing factor to his rhythmic movement disorder. Of interest, the patient had long sleep latency and overall short duration of sleep on the in-lab polysomnogram, and this was felt to represent first night effect in the sleep laboratory.
Children with mild or intermittent symptoms do not require treatment and the majority will outgrow the condition. Treatment is indicated if there is significant daytime impairment or concern for bodily injury. There are no evidence-based treatment guidelines at present, however, a low dose of a benzodiazepine or a selective serotonin reuptake inhibitor has been used. Other treatment options include sleep restriction, hypnosis and behavioral modifications (7).
Answers
-
The most likely diagnosis is sleep-related rhythmic movement disorder.
-
The most appropriate next step in the management of this patient was reassurance and discussion of safety measures.
Follow-Up
This patient was seen by a pediatric neurologist who obtained a sleep-deprived EEG to suggest any underlying seizure tendencies. The EEG was normal.
Reassurance, safety measures, and improved sleep hygiene were recommended. The patient’s sleep apnea was very mild and watchful waiting was decided after a thorough discussion with the family.
References
-
American Academy of Sleep Medicine. International classification of sleep disorders 3rd ed. Darien, IL:2014
-
Laberge L, Tremblay RE, Vitaro F, et al. Development of parasomnias from child hood to early adolescence. Pediatrics. 2000;106(1 pt 1):67-74
-
American Academy of Sleep Medicine. The AASM manual for scoring of sleep and associated events: rules terminology and technical specifications. Version 2.1; Darien IL: 2014
-
Mayer G, Wilde-Frenz J, Kurella B. Sleep related rhythmic movement disorder revisited. J Sleep Res 2007;16:110-6
-
Dyken ME, Lin-Dyken DC, Yamada T. Diagnosing rhythmic movement disorder with video polysomnography. Pediatr Neurol. 1997;16:37-41
-
Manni R, Terzaghi M. Rhythmic movements during sleep: a physiological and pathological profile. Neurol Sci 2005;26:s181-5
-
Manni R, Tartara A. Clonazepam treatment of rhythmic movement disorders. Sleep. 1997;20:812


