Contributed by Gaurav Nigam MD1, Muhammad Riaz MD1, Neeraj Kaplish MD1 1University of Michigan Sleep Disorders Center, Ann Arbor, Michigan Corresponding Author: Gaurav Nigam, MD Michael S. Aldrich Sleep Disorders Laboratory 1500 East Medical Center Drive, Ann Arbor, MI 48109-5845 Email: dr.nigamgaurav@gmail.com
In Brief
A middle-aged woman with progressive multiple sclerosis presented to a sleep clinic for evaluation of insomnia, snoring and morning headaches. Polysomnography showed an unanticipated pattern of sleep disordered breathing which resolved in response to treatment with a newer type of ventilatory assistive device.
Case Vignette
A 58-year-old female with secondary progressive multiple sclerosis and insomnia presented to a sleep disorders clinic with snoring and morning headaches. She had no suggestive symptoms or history of congestive heart failure. Also, she had no history of stroke, chronic kidney disease or use of opioid medications.
Overnight in-laboratory polysomnography was performed. The hypnogram is shown in
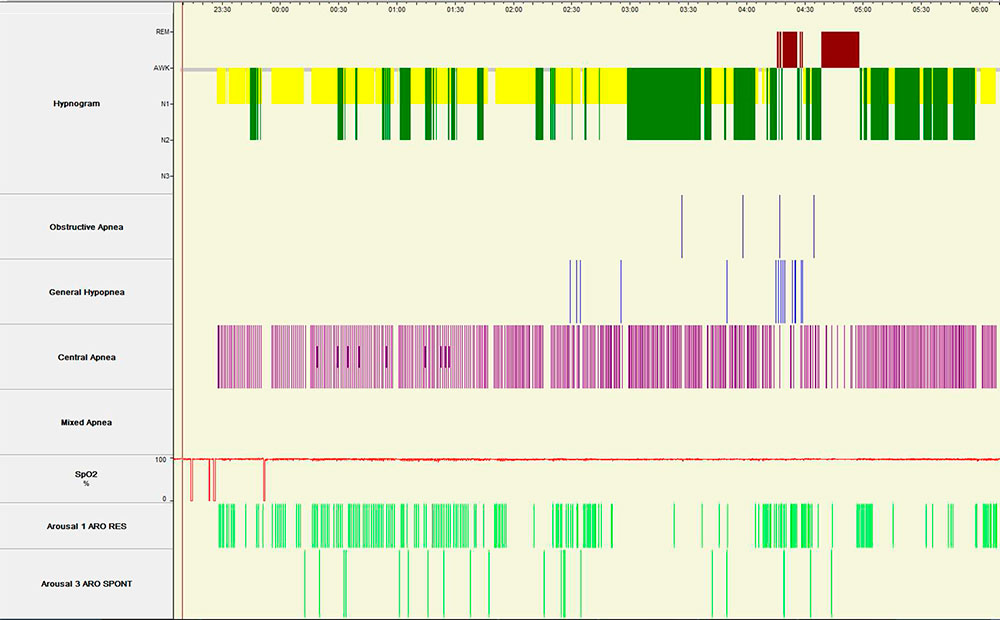
Figure 1

Figure 2
A recent brain and cervical spine MRI was reviewed (Figure 2). This was suggestive of extensive demyelination as demonstrated by scattered, irregular and patchy lesions of T2 and fluid attenuated inversion recovery (FLAIR) hyperintensity seen in the deep and periventricular white matter of the bilateral cerebral hemispheres, representing demyelinating plaques. Additional nodular lesions were seen in the brainstem and the bilateral cerebellar white matter. There was no evidence of pathologic enhancement or restricted diffusion in any of the lesions.
Question:
-
Can multiple sclerosis be associated with central sleep apnea in a Cheyne-Stokes breathing pattern?
-
Can other central nervous system demyelinating diseases similar to multiple sclerosis cause central sleep apnea in a Cheyne-Stokes breathing pattern?
-
Is adaptive servo ventilation an effective treatment modality for central sleep apnea with Cheyne-Stokes breathing in such patients without known heart failure?
Diagnosis
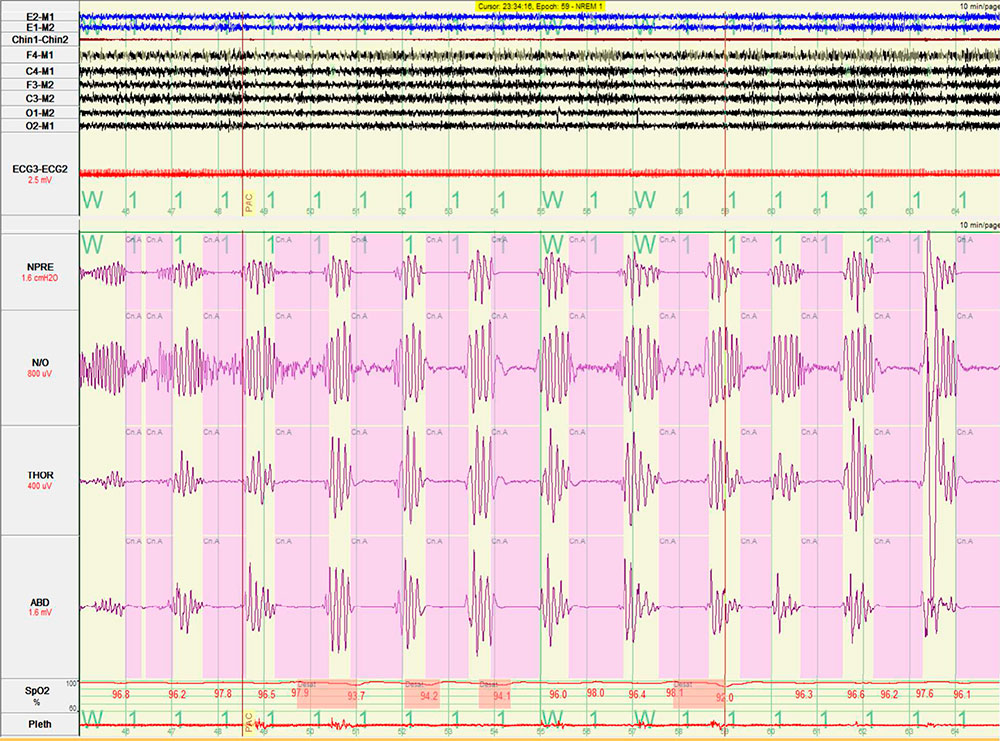
Figure 3
An attended in-lab diagnostic polysomnogram demonstrated primarily central sleep apnea with an apnea hypopnea index (AHI) of 78, a central apnea index (CAI) of 75, and a Cheyne-Stokes breathing pattern (Figure 3).
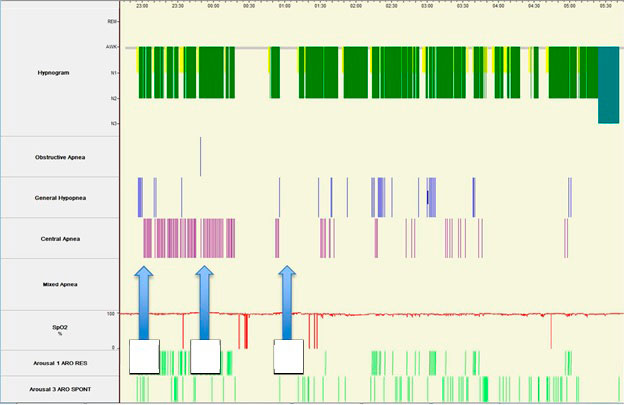
Figure 4
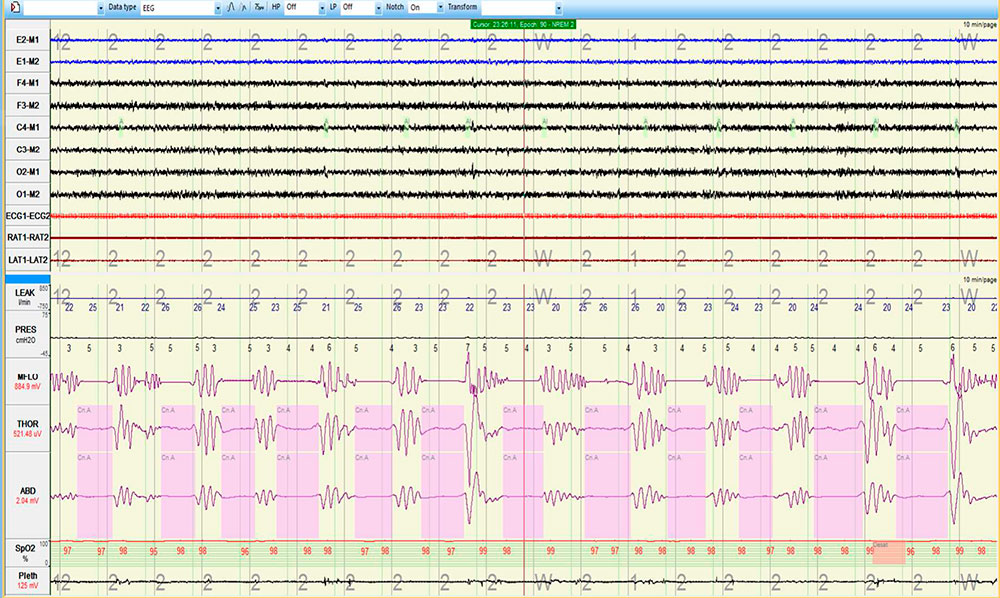
Figure 5

Figure 6
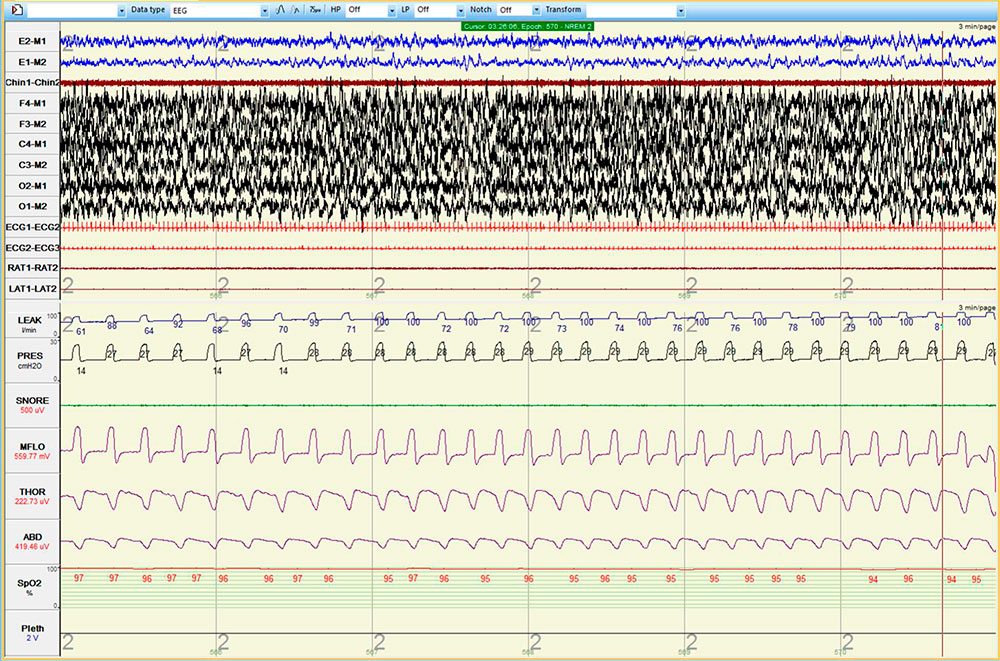
Figure 7
The patient underwent a single night titration study with the intent of abolishing the abnormal breathing pattern (Figure 4). Because abnormal breathing persisted on CPAP (Figure 5), bi-level PAP titration was tested next. Bi-level PAP also failed to ameliorate abnormal breathing (Figure 6). A subsequent trial of adaptive servo ventilation led to near complete resolution of central sleep apnea with Cheyne-Stokes breathing (Figure 7).
Discussion
Central sleep apnea with Cheyne-Stokes breathing is common in patients with heart failure, stroke, or renal failure, but has not been reported in patients with multiple sclerosis to our knowledge (1-3). Demyelinating lesions in the brainstem often predispose multiple sclerosis
patients to develop severe central sleep apnea, which was prominent in this case (4) (Figure 2).
It is plausible that extensive demyelination in this patient’s ponto-medullary pacemaker as well as other brainstem nuclei regulating respiration caused her Cheyne-Stokes breathing pattern on a backdrop of central sleep apnea. It remains to be seen whether other demyelinating disorders such as Guillain-Barre syndrome and chronic inflammatory demyelinating neuropathy can have similar polysomnographic manifestations.
This clinical case draws attention to the fact that multiple sclerosis patients with significant demyelination within the brainstem can have central sleep apnea with Cheyne- Stokes breathing even in the presence of snoring. This case also highlights the limitations of home sleep studies for patients with demyelinating neurological disorders since their capability to detect central apneas remains uncertain (5). Maintaining a high index of clinical suspicion and ordering an attended in-lab polysomnogram may be necessary to demonstrate co-existing central sleep apnea with Cheyne-Stokes breathing in some patients with extensive demyelinating disease.
Adaptive servo ventilation provided this patient with effective control of her sleep disordered breathing. This observation merits further investigation of this type of mechanical respiratory assistance for selected patients with sleep disordered breathing caused by multiple sclerosis.
Answers
-
Multiple sclerosis can be associated with central sleep apnea in a Cheyne-Stokes breathing pattern depending on the location of brainstem lesions and severity of the central sleep apnea.
-
It remains to be seen if other demyelinating disorders such as Guillain- Barre syndrome and chronic inflammatory demyelinating neuropathy can sometimes have similar polysomnographic manifestations.
-
Adaptive servo ventilation may prove generally effective in treating multiple sclerosis patients with central sleep apnea accompanied by Cheyne-Stokes breathing.
References
-
International Classification of Sleep Disorders, 3rd ed, American Academy of Sleep Medicine, Darien, IL 2014.
-
Brack T, Randerath W, Bloch KE. Cheyne-Stokes respiration in patients with heart failure: prevalence, causes, consequences and treatments. Respiration 2012;83:165-176.
-
Braley TJ, Segal BM, Chervin RD. Sleep-disordered breathing in multiple sclerosis. Neurology 2012;79:929-936.
-
Fleming WE, Pollak CP. Sleep disorders in multiple sclerosis. Semin Neurol 2005;25:64-68.
-
Collop NA, Anderson WM, Boehlecke B, Claman D, Goldberg R, Gottlieb DJ, Hudgel D, Sateia M, Schwab R, Portable Monitoring Task Force of the American Academy of Sleep Medicine. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. Portable Monitoring Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med 2007;3:737-747.


