Contributed by Mudiaga O. Sowho1, Erica Wolfe1, Emi Z. Murano2, Jason P. Kirkness1 1Johns Hopkins Sleep Disorders Center, Division of Pulmonary and Critical Care Medicine, Johns Hopkins School of Medicine, Baltimore, MD; 2The Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins School of Medicine, Baltimore, MD Corresponding Author: Mudiaga O. Sowho MD, MPH, Johns Hopkins Sleep Disorders Center, Division of Pulmonary and Critical Care Medicine, 5501 Hopkins Bayview Circle, Asthma & Allergy Building, Baltimore, MD 21224, Tel: (410) 550-2026; Fax: (410) 550-3374, E-mail: msowho1@jhmi.edu Running Head: Vibrato, Tremolo or Upper Airway Oscillation Keywords: Essential tremor, Flow oscillations, Sleep apnea, Myoclonus, Upper Airway Grants: This study is supported by American Hearts Association Grant no: 12SDG8100000. Disclosures: No conflicts of interest, financial or otherwise, are declared by the author(s).
In Brief
We describe a case of a 48 year old woman with an incidental finding on a research polysomnogram, which posed an interesting differential diagnosis elucidated with the aid of advanced diagnostic methods. This case illustrates the utility of quantitative airflow assessment during sleep in the evaluation of involuntary upper airway phasic activity.
Case Vignette
A 48 year-old African-American woman presented for an overnight polysomnography study as part of participation in a research protocol. Although the patient had no prior complaints, on the screening questionnaire, she acknowledged loud snoring and mouth dryness upon awakening. Her screening physical examination was significant for narrowed lateral pharyngeal arch, Mallampati grade IV airway and audible staccato breathing during expiration. The rest of her examination was unremarkable. She had a traumatic incident 16 years ago that required hospitalization for splenic repair. She admits that there was brief loss of consciousness following trauma but had no other neurologic symptoms.
The polysomnogram revealed a sleep latency of 5 minutes; both, decreased slow wave and REM sleep, with a slightly decreased sleep efficiency (74.9%). The total, NREM and REM apnea–hypopnea index (AHI) were 6.2 events/hr, 1.2 events/hr and 47 events/hr respectively. Similarly, the total, NREM and REM arousal index (AI) were 11.3 events/hr,12.7events/hr and 26.1 events/hr. All of the respiratory events were obstructive. The minimum O2 saturation was 84% during NREM sleep and 88% during REM sleep. Airflow tracing showed rhythmic phasic oscillations during wake and sleep. Oscillations persisted during NREM and REM sleep with similar frequency and amplitude, and were only absent in apnea (Figure1).
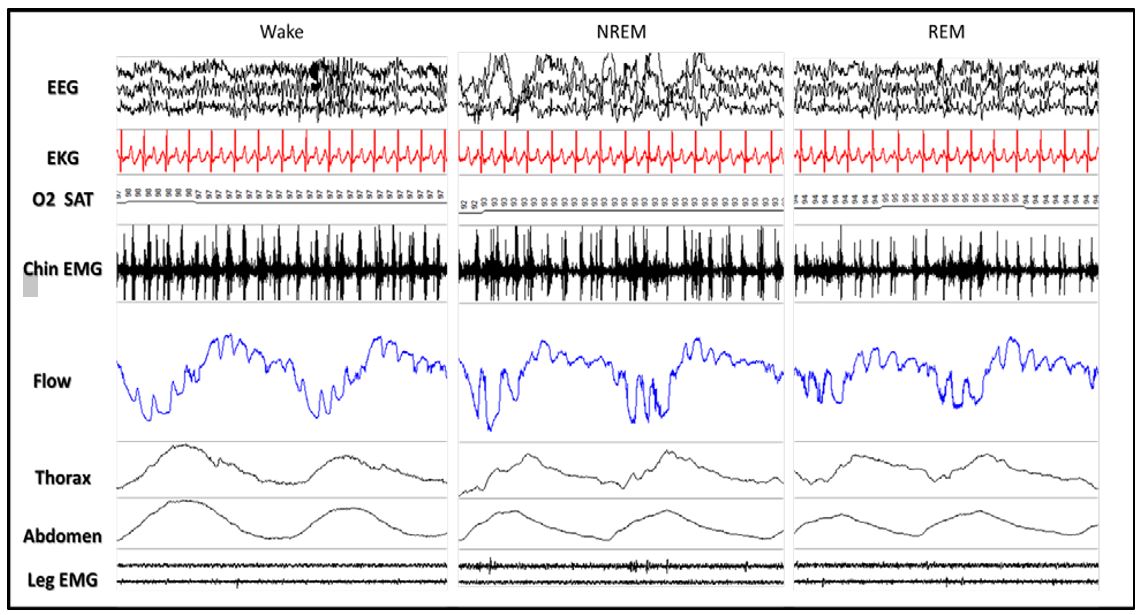
Figure 1: Two-breath cycles in Wake, NREM and REM sleep. Polysomnogram includes EEG, EKG, oxygen saturation, airflow, thoracic effort, abdominal effort and leg EMG channels. Flow oscillations persist during wake and sleep, as well as during inspiration and expiration.
We noticed subtle quivers in her speech during sustained phonation and she subsequently had a dynamic MRI of the upper airway, obtained as part of research. The MRI did not show any aberrant upper airway tissue or mass; however, bilateral rhythmic movements of the palatal, pharyngeal and laryngeal walls were noted. The MRI findings are shown below.
Question
Based on the clinical vignette, polysomnogram and MRI findings, what is the diagnosis?
Discussion
Voice tremor is the phonatory manifestation of the essential tremor syndrome, characterized by involuntary skeletal muscle contraction that leads to oscillatory movement of laryngeal muscles at a rate of 4-10 Hz (1). There is wide disparity in symptom severity, with severe forms presenting as audible dysphonia and mild cases undetected or mere incidental findings (2). In some cases, the muscles of the palate and pharynx are seen to synchronously oscillate with the larynx (3).This kind of upper airway involvement can lead to rapid intermittent changes in airway resistance with continuous interruption in airflow (4).
Persistent Oscillations in Airflow Signal
In this patient, the airflow tracing from the polysomnograph, showed oscillations at a rate of 2.2 Hz during both, inspiratory and expiratory phases (Figure 1). Airflow oscillations continue throughout the study, except during apneas, although rapid phasic bursts in chin EMG signal persist at the same frequency as the fluctuations in flow. At first, we ruled out artifacts that could affect the airflow tracing, such as humming (50-60 Hz), cardioballistic airflow (frequency most commonly < 1.5 Hz) and channel cross-talking between ECG (1.33 Hz or 80bpm) and EMG channels (Figure 2). Salas et al, described a case of idiopathic palatal myoclonus with demonstrable flow oscillations from polysomnography (7). Conditions in the differential, such as Shy-Drager syndrome and other extrapyramidal disorders may also result in flow oscillations during wakefulness (8), but do not persist during sleep.
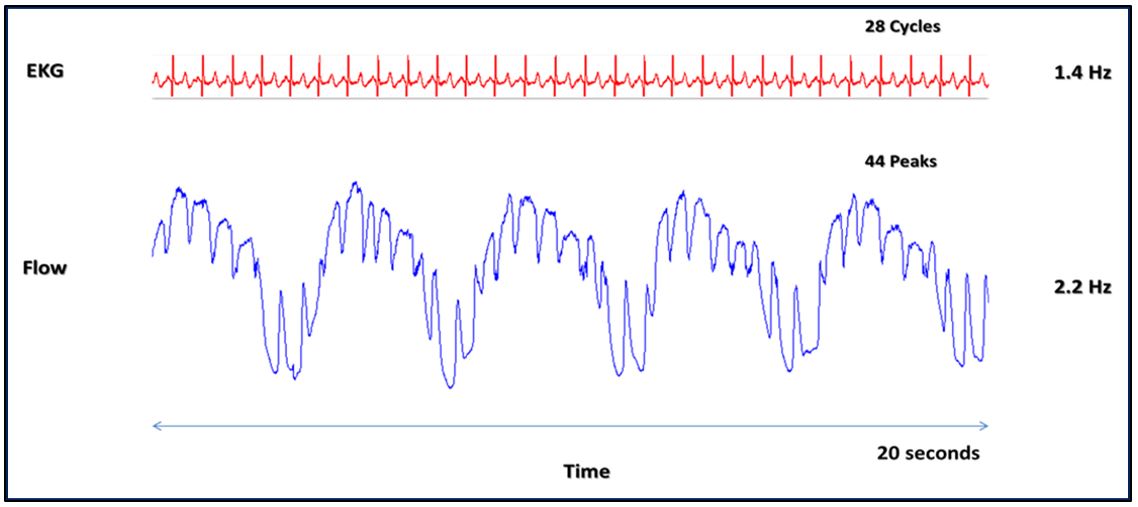
Figure 2: Twenty second epoch displaying the EKG and airflow channel. The frequency of the cardiac rhythm (1.4 Hz) is shown to be slower than the flow oscillations (2.2 Hz).
Evaluation and Diagnosis
A 3D dynamic MRI of the upper airway performed during wakefulnessat 18 frames per second,as part of research, showed involuntary elevation of the soft palate, tongue movements anteriorly, and adduction of the palato-pharyngo-laryngeal walls. The upper airway structures demonstrated rhythmic contraction during rest and continuous phonation at the same frequency (2.2 Hz) as seen in the polysomnographic airflow signal. In the clinical setting, laryngoscopy would be the first procedure in the workup for subtle upper airway closure; however, the advantage of utilizing 3D MRI provided the ability to visualize the entire airway simultaneously.
We believe the EMG bursting signals throughout the polysomnograph to represent one or a combination of any of the mouth floor and tongue muscles, since rhythmic movements of hyoid bone anteriorization (genioglossus), tongue twitching (genioglossus) and tongue elevation (mylohyoid) (5) were clearly visualized on the MRI at rest (video). In the polysomnogram, we measured airflow using a full face mask and a pneumotachograph that could quantify the airflow insufficiency associated with airway closure oscillation. Airflow measurements, revealed an 80-90% decrease in both inspired and expired airflow rate during oscillations. We suspect that this may interact with upper airway collapse and sleep disordered breathing, although we don’t know if this is intrinsically related to her sleep apnea per se. Airflow oscillations occurred throughout the night except during complete upper airway obstruction (Figure 3) suggesting that oscillations take place at or below the site of obstruction. Persistence of the low frequency EMG spikes (Figure 3) suggests that the underlying muscle contractions continue during apnea.

Figure 3: Forty five second epoch showing an apneic event-related oxygen desaturation during REM sleep. The EMG and airflow channels are duplicated to show the persistence of inspiratory phase high frequency (>30 Hz) activity after low frequency filtering. Low frequency oscillations (<3Hz) occur in both inspiratory and expiratory limbs of the flow signal, and also continue in the EMG channel during apnea.
Conclusion
Semi-quantitative instrumentation, such as nasal cannula or thermistors may have inadequate sensitivity for routinely characterizing airflow oscillations as described. Measurement of airflow during sleep could indeed become a neuro-topological biomarker and a valuable tool in the evaluation of involuntary upper airway phasic activity, providing physicians with a quantitative and qualitative means for characterizing the presence and intensity of abnormal muscle rhythmicity (6).
The current volunteer would benefit from a complete neurologic and ENT assessment to further characterize the research findings.
Answer
Essential upper airway muscles’ tremor with mild obstructive sleep apnea.
This patient’s PSG demonstrated snoring, mild apnea with a total AHI of 6.2 and persistent flow oscillations in both wake and sleep. The amplitude and frequency of oscillations are preserved in NREM and REM. Rhythmic pattern persists in inspiration, expiration, flow limited breathing but absent in apnea. An involuntary rhythmic elevation of the soft palate, concentric medialization of the pharyngeal wall, elevation of the hyoid bone, laryngeal complex and twitching of the tongue were simultaneously seen on the real-time dynamic MRI at 18 frames per second.
Together these examination findings are consistent with an essential tremor syndrome; in this case, upper airway muscles’ tremor with mild sleep disordered breathing. However, a very close differential that has been considered is palato-pharyngo-laryngeal myoclonus.
References
- Lederle, A., J. Barkmeier-Kraemer, and E. Finnegan. "Perception of vocal tremor during sustained phonation compared with sentence context." J.Voice 26.5 (2012): 668-69.
- Lester, R. A., J. Barkmeier-Kraemer, and B. H. Story. "Physiologic and acoustic patterns of essential vocal tremor." J.Voice 27.4 (2013): 422-32.
- Wolraich, D., et al. "Laryngeal tremor: co-occurrence with other movement disorders." ORL J.Otorhinolaryngol.Relat Spec. 72.5 (2010): 291-94.
- Vincken, W. G. and M. G. Cosio. "Flow oscillations on the flow-volume loop: clinical and physiological implications." Eur.Respir.J. 2.6 (1989): 543-49.
- Bogart BI, Ort VH. Elsevier’s integrated anatomy and embryology. Mosby, 2007.
- Katz, I., et al. "An evaluation of flow-volume curves as a screening test for obstructive sleep apnea." Chest 98.2 (1990): 337-40.
- Salas, R., et al “Concurrent presentation of palatal myoclonus and sleep apnea: A polysomnographic assessment”. Sleep Med. 2009 Dec; 10(10):1163-6.
- Drysdale, A. J., J. Ansell, and J. Adeley. "Palato-pharyngo-laryngeal myoclonus: an unusual cause of dysphagia and dysarthria." J.Laryngol.Otol. 107.8 (1993): 746-47.


