Contributed by Pedro R. Genta1,2, Francisco M. Oliveira2, and Sidney Gomes2 1Pulmonary Division, Heart Institute (InCor)/Hospital das Cl´ınicas, University of São Paulo School of Medicine, and 2Hospital Beneficeˆ ncia Portuguesa de São Paulo, São Paulo, Brazil
In Brief
A sleep medicine consultation was requested for an elderly male patient with nocturnal epilepsy, agitated sleep, and snoring. In-hospital polysomnography was performed.
A 77-year-old man was admitted because of recurrent tonic-clonic seizures during sleep. He had a past medical history of temporal lobe epilepsy diagnosed 7 years previously that was characterized by complex partial and generalized tonic-clonic seizures. Sleep medicine consultation was requested because his seizure episodes had become increasingly more common during sleep. The nocturnal seizure episodes were first noticed 2 years previously but had worsened in frequency during the previous month (almost every night). He also had seizures during the day, which were unchanged in frequency (twice a week). His daytime complex partial seizures were characterized by feelings of fear and anger, vertigo, tachycardia, and dilated pupils that usually evolved to complex automatisms and dystonic movements of the right upper limb. A generalized tonic-clonic seizure usually followed. He denied a family history of epilepsy. His wife stated that the patient snored frequently and loudly, had agitated sleep and frequent awakenings. His Epworth Sleepiness Scale score equaled 6. He was also being treated for ischemic heart failure, hypertension, and gastroesophageal reflux disease. His current medications were isosorbide mononitrate, metoprolol, hydralazine, carbamazepine (1,800 mg/d), domperidone, and omeprazole.
His body mass index was 31 kg/m2 and his Mallampati score was IV. Polysomnography was performed in the patient’s hospital room. His apnea– hypopnea index was 40 events/hour (118 apneas: 109 obstructive, 1 mixed, and 8 central; and 75 hypopneas). The lowest oxygen saturation was 72%. An electroencephalographic abnormality and an associated respiratory event were registered and are shown in Figure 1.
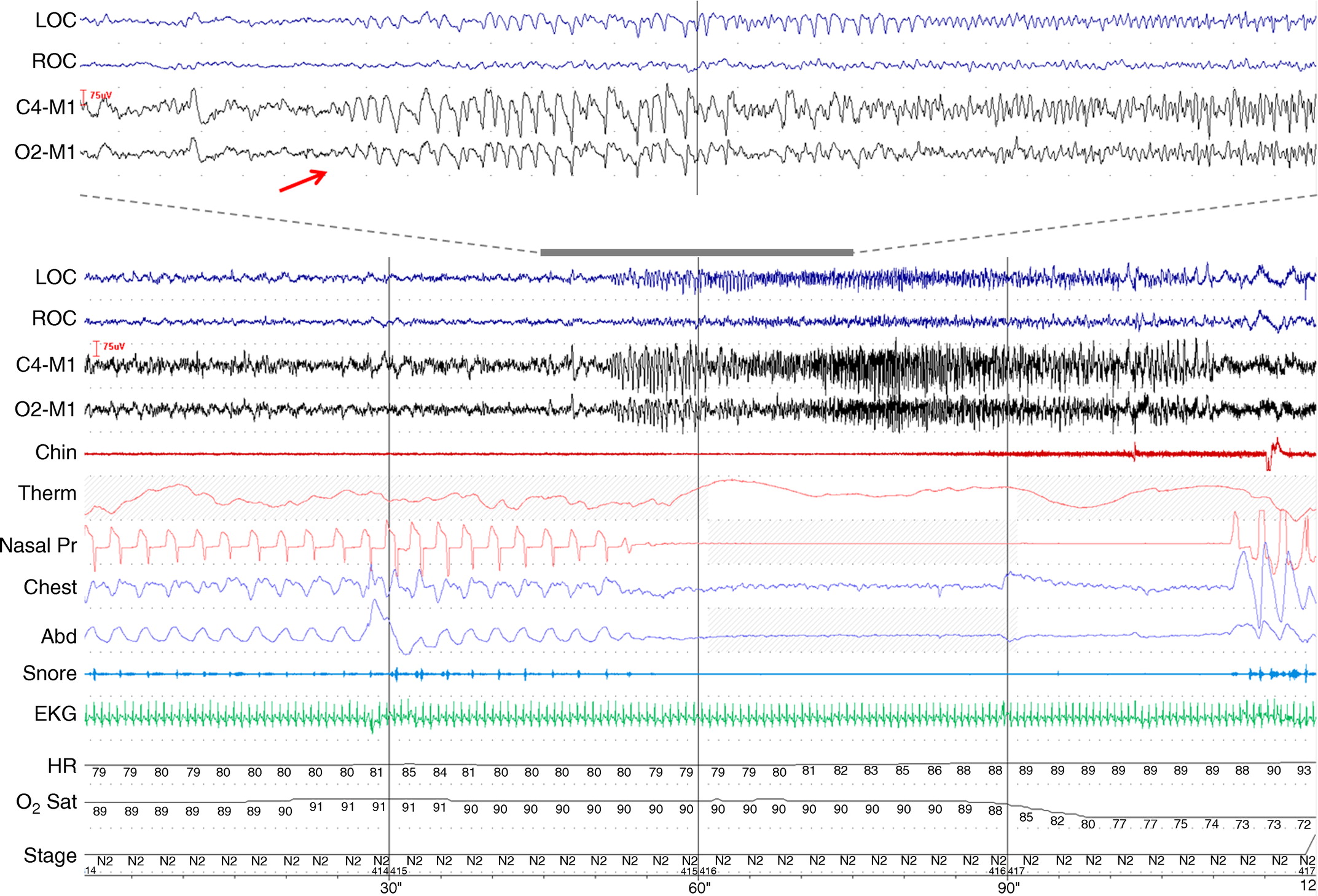
Figure 1. Sleep tracing from the in-hospital patient’s polysomnography recording. Bottom: 2 minutes. Top (close-up): 30 seconds. Red arrow indicates onset of ictal epileptiform activity. C4-M1 and O2-M1 = electroencephalogram; Chest and Abd = chest and abdominal bands; Chin = submental electromyogram; EKG = electrocardiogram; HR = heart rate; LOC and ROC = left and right electrooculogram, respectively; N2 = stage 2; Nasal Pr = nasal pressure cannula; O2 sat = oxygen saturation; stage = sleep stage; Therm = oronasal thermistor.
Questions
-
What electroencephalographic abnormality is shown in Figure 1?
-
What type of respiratory event is associated with the EEG abnormality in Figure 1?
Discussion
The patient had a tonic-clonic seizure during the polysomnography (Figure 1), where ictal epileptiform activity is characterized by abrupt onset (Figure 1, red arrow) and repetitive and rhythmic waveforms with varying frequency. A prolonged (60 s) central apnea followed the seizure episode, leading to an oxygen saturation of 72%. However, the majority of events during the polysomnography were obstructive and obstructive sleep apnea (OSA) was diagnosed. Central apnea is the most common type of apnea during seizure episodes (1, 2). The mechanisms for the occurrence of central apneas during seizures are not known but are possibly related to central respiratory control suppression during the seizure discharge.
The characteristics of the central apnea shown in Figure 1 are somewhat different from central apneas that follow obstructive events and those associated with Cheyne- Stokes and idiopathic central apnea (3). In these circumstances, central sleep apneas are generally preceded by a period of hyperventilation, have a shorter duration (10–20 s), and usually do not lead to significant oxygen desaturation (3). In the present case, the patient had two different types of central events. He had seven central apneas that followed obstructive events and were short in duration (11 s on average), leading to mild desaturation (3% on average). The other type of central apnea presented by this patient was the one associated with the seizure episode, which was considerably longer (60 s) and led to profound oxygen desaturation (18%) (Figure 1).
The relationship between epilepsy and sleep is complex and bidirectional. Nocturnal epilepsy may lead to sleep fragmentation and daytime sleepiness (4). OSA may aggravate epilepsy because of recurrent oxygen desaturation, sleep deprivation, and decrease in deeper stages of sleep. Seizures of frontal lobe origin are more likely to occur during sleep than wakefulness. However, seizures of temporal, parietal, or occipital lobe origin are generally more common during wakefulness (5). Regarding sleep stage predominance, most seizures occur during non-REM sleep (5). We used a simplified EEG montage for this patient to investigate possible OSA. However, in-laboratory polysomnography with extended EEG montage and video recording should be considered to investigate nocturnal epilepsy.
A high prevalence of OSA has been reported among patients with epilepsy (6, 7). OSA is a common comorbidity among adults with late-onset or worsening seizures (7). Data derived from a few small studies suggest that OSA treatment can reduce epileptiform discharges and seizure frequency (8–10). However, larger controlled studies assessing the benefit of OSA treatment in patients with epilepsy are needed.
In conclusion, this case illustrates a central apnea associated with a seizure episode, characterized by prolonged duration and pronounced desaturation.
Answers
- What electroencephalographic abnormality is shown in Figure 1?
Ictal epileptiform activity. - What type of respiratory event is associated with the EEG abnormality in Figure 1? Central apnea is the most common type of apnea during seizure episodes.
Follow-Up
During hospitalization, the carbamazepine dose was increased to 2,000mg and clobazam10 mg was added. The patient agreed to start nasal continuous positive airway pressure (CPAP), which was titrated to 10 cm H2O. At 4 months of follow-up, he was using CPAP regularly. His daytime and nocturnal seizure frequency significantly improved (,1 episode/month). Sleep quality also improved substantially.
Author disclosures are available with the text of this article at www.atsjournals. org.
References
-
Pavlova M, Singh K, Abdennadher M, Katz ES, Dworetzky BA, White DP, Llewellyn N, Kothare SV. Comparison of cardiorespiratory and EEG abnormalities with seizures in adults and children. Epilepsy Behav 2013;29:537–541.
-
Ryvlin P, Nashef L, Lhatoo SD, Bateman LM, Bird J, Bleasel A, Boon P, Crespel A, Dworetzky BA, Høgenhaven H, et al. Incidence and mechanisms of cardiorespiratory arrests in epilepsy monitoring units (MORTEMUS): a retrospective study. Lancet Neurol 2013; 12:966–977.
-
Hall MJ, Xie A, Rutherford R, Ando S, Floras JS, Bradley TD. Cycle length of periodic breathing in patients with and without heart failure. Am J Respir Crit Care Med 1996;154:376–381.
-
Vaughn BV, Ali I. Sleep and epilepsy: opportunities for diagnosis and treatment. Neurol Clin 2012;30:1249–1274.
-
Bazil CW, Walczak TS. Effects of sleep and sleep stage on epileptic and nonepileptic seizures. Epilepsia 1997;38:56–62.
-
Phillips MC, Costello CA, White EJ, Smit M, Carino J, Strawhorn A, Jackson B, Kwan P, French CR, Yerra SR, et al. Routine polysomnography in an epilepsy monitoring unit. Epilepsy Res 2013;105:401–404.
-
Chihorek AM, Abou-Khalil B, Malow BA. Obstructive sleep apnea is associated with seizure occurrence in older adults with epilepsy. Neurology 2007;69:1823–1827.
-
Vendrame M, Auerbach S, Loddenkemper T, Kothare S, Montouris G. Effect of continuous positive airway pressure treatment on seizure control in patients with obstructive sleep apnea and epilepsy. Epilepsia 2011;52:e168–e171.
-
Malow BA, Weatherwax KJ, Chervin RD, Hoban TF, Marzec ML, Martin C, Binns LA. Identification and treatment of obstructive sleep apnea in adults and children with epilepsy: a prospective pilot study. Sleep Med 2003;4:509–515.
-
Oliveira AJ, Zamagni M, Dolso P, Bassetti MA, Gigli GL. Respiratory disorders during sleep in patients with epilepsy: effect of ventilatory therapy on EEG interictal epileptiform discharges. Clin Neurophysiol 2000;111:S141–S145.


