Contributed by Melissa Carlucci, MS, APN; Bharati Prasad, MD Sleep Science Center University of Illinois at Chicago Chicago, Illinois Melissa Carlucci, MS, APN Clinical Instructor Department of Biobehavioral Health Science University of Illinois at Chicago College of Nursing
An 84-year old woman presented with excessive daytime sleepiness (EDS) dating back to the onset of her retirement from work 2 decades ago. Her daytime sleepiness had become more severe over the previous 5 years. Additional relevant symptoms included snoring and difficulty maintaining sleep. She described a regular sleep schedule with 7 to 8 hours of sleep most nights and without daytime naps. Other medical diagnoses included hypertension, diabetes, osteoarthritis, and goiter. Her current medications included aspirin, amlodipine, lisinopril, metformin, and cyclobenzaprine, and hydrocodone taken as needed.
The patient’s Epworth Sleepiness Scale (ESS) score was 11/24. Her body mass index (BMI) was 36, and her neck circumference was 17 inches. She had a Mallampati class III oropharynx. Recent magnetic resonance imaging of the brain showed age-related changes with no identified focal abnormalities.
An attended, in-laboratory polysomnogram (PSG) showed sleep efficiency of 63.5%, an apnea hypopnea index (AHI) of 0.9 per hour, a periodic limb movement index of 0.0 per hour, and no EEG or ECG abnormalities. Rapid eye movement (REM) latency was two minutes.
At the time of a subsequent office visit, she described occasional sleep paralysis and two recent brief episodes of falling to the floor without associated loss of consciousness. The first episode occurred while she was standing and watching a tennis match on television; the second took place while she was sitting and playing a computer game.
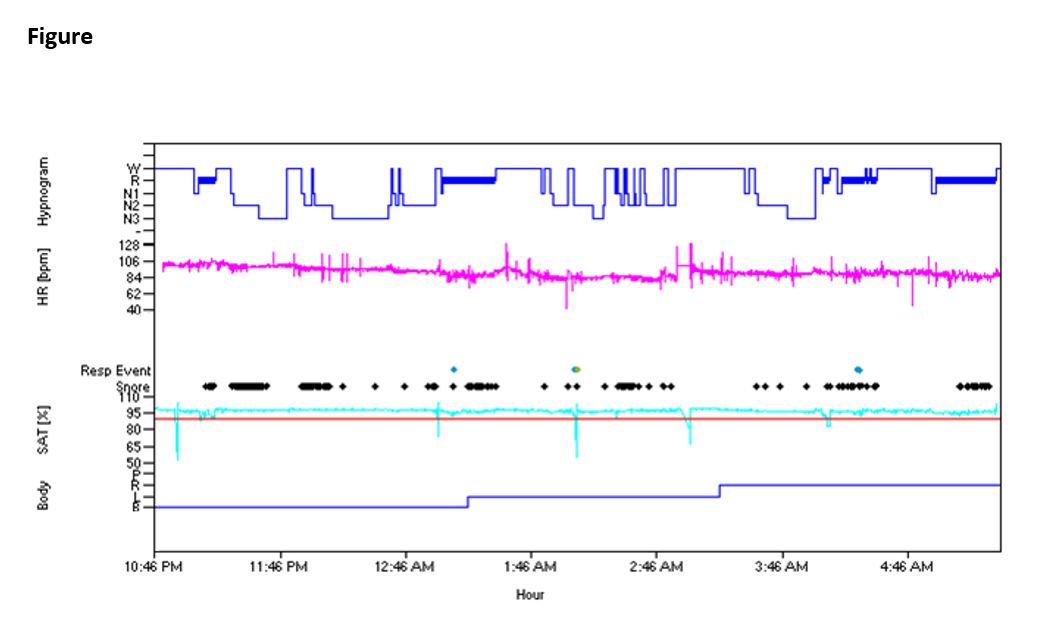
Figure Legend
A hypnogram from the patient’s baseline polysomnogram
| W = wake | SAT (%) = oxygen saturation |
| R = REM | Body = body position |
| N1 = NREM stage 1 | P = prone |
| N2 = NREM stage 2 | R = right side |
| N3 = NREM stage 3, slow wave sleep | L = left side |
| HR (bpm) = heart rate (beats per minute) | B = back |
| Resp Events = respiratory events |
Questions:
What is the best next study to diagnose her sleep disorder?
What is the most likely diagnosis?
Discussion:
Although her history of snoring, a BMI of 36, a neck circumference of 17, and a Mallampati class III oropharynx raised initial suspicion of obstructive sleep apnea, that diagnosis was eliminated by a low AHI on her polysomnogram. As a next diagnostic study, consideration was given to performing urine toxicology screening to look for illicit substance use as a possible explanation for her excessive daytime sleepiness. However, this patient was deemed a reliable and consistent historian, and illicit drug use was not documented in her medical record and was considered unlikely in an 84-year old woman. A request that the patient keep a sleep diary to document her sleep-wake cycles was also considered. However, her self-reported sleep schedule was regular, her reported sleep nightly duration was sufficient, and she seemed reliable.
Our attention then turned to the early onset of REM sleep documented on her polysomnogram (Figure) and to the history suggestive of recent cataplexy episodes. Our next diagnostic study was a multiple sleep latency test (MSLT). Sleep continuity and sleep architecture from the preceding polysomnogram are presented in Table 1. The results of the MSLT, presented in Table 2, confirmed a diagnosis of narcolepsy.
Table 1
Polysomnogram Sleep Continuity and Sleep Architecture
|
Lights Out |
11:02 PM |
|
Lights On |
7:30 AM |
|
Time in Bed |
508 minutes |
|
Total Wake Time |
149 minutes |
|
Total Sleep Time |
359 minutes |
|
% Stage N1 |
12% |
|
Sleep Efficiency |
71% |
|
% Stage N2 |
47% |
|
Sleep Latency |
7 minutes |
|
% Stage N3 |
24% |
|
REM Latency |
70 minutes |
|
% Stage REM |
17% |
Table 2
Multiple Sleep Latency Test
|
|
Sleep Latency (minutes) |
REM Latency (minutes) |
|
Nap 1 |
12.5 |
3 |
|
Nap 2 |
4 |
8.5 |
|
Nap 3 |
8.5 |
N/A |
|
Nap 4 |
3 |
7 |
|
Nap 5 |
10 |
N/A |
Mean Sleep Latency: 7.6
Number of SOREMPs: 3
Narcolepsy is a disorder of the sleep-wake cycle that is characterized by a disturbance in rapid eye movement (REM) sleep. This presents clinically with excessive daytime sleepiness (EDS) and manifestations of impaired REM sleep, which may include cataplexy, hypnagogic or hypnopompic hallucinations, and sleep paralysis (1). The first expression of symptoms of narcolepsy typically occurs during the second or third decade of life. Often, the first symptom is EDS (2). Cataplexy occurs in more than half of patients with narcolepsy (1,2) and is highly specific for this disease (3). Some patients experience their first episode of cataplexy near the onset of EDS (2); most others report the onset of cataplexy within five years after the onset of EDS (3). However, delays of twenty years or more in the expression of cataplexy can occur (1,3). Although the first symptoms of narcolepsy typically occur before the age of 30, the disease is not diagnosed until after the age of 40 in approximately half of patients (4).
A history of EDS and cataplexy combined with a positive multiple sleep latency test (MSLT) is considered diagnostic for narcolepsy with cataplexy. An MSLT is positive for narcolepsy if the mean sleep latency is eight minutes or less and REM sleep begins within 15 minutes after the onset of sleep on 2 or more occasions (5). These latter events are called sleep-onset REM periods (SOREMPs).
The onset of narcolepsy in an older adult is uncommon, but there have been reported cases of symptom onset up to the eighth and ninth decades of life (3,6). The expression of narcolepsy in older adults may be different than in their younger counterparts. In narcoleptic patients aged 60 and older, cataplexy is more likely to present before EDS (2) and can be a cause of falls (3). However, episodes of cataplexy may also decrease with age (1,7). Diagnosing narcolepsy in an older adult can be challenging, as there may be a decrease in the frequency of SOREMPs and an increase in mean sleep latency as a function of age (7). In addition, older adults are more likely to have medical comorbidities or be taking medications that could affect sleep and the expression of narcolepsy symptoms (3). Narcolepsy is a chronic, but generally not progressive disease. Mild severity of EDS or late onset of cataplexy can contribute to misdiagnosis or a delay in diagnosis (4,6).
Our patient was first given a diagnosis of narcolepsy with cataplexy at age 84. Notably, her Epworth Sleepiness Scale (ESS) score was only 11 at presentation. There is a poor correlation between ESS and mean sleep latency on MSLT (8). Although she had been experiencing sleepiness for approximately 20 years, her first episode of cataplexy did not occur until a few months prior to her presentation. As illustrated by this case, narcolepsy should be considered in the differential diagnosis of EDS, regardless of age.
AnswersThe best next study was a Multiple Sleep Latency Test (MSLT)
The diagnosis is late-onset narcolepsy
Insights
- Although typically a disease of younger adults, narcolepsy can present in patients after the age of 60. This diagnosis can be challenging in older adults.
- In older adults, cataplexy often presents before the onset of excessive daytime sleepiness and can be the cause of falls.
References:
- Guilleminault C, Cao MT. Chapter 85 narcolepsy: diagnosis and management. In: Kryger MH, Roth T, Dement, WC, editors. Principles and practice of sleep medicine, 5th ed. St. Louis, MO: Elsevier Saunders; 2011.
- Ohayon MM, Ferini-Strambi L, Plazzi G, Smirne S, Castronovo V. How age influences the expression of narcolepsy. J Psychosom Res 2005; 59(6): 399-405.
- Chakravorty SS, Rye DB. Narcolepsy in the older adult. Drugs Aging 2003; 20(5): 361-376.
- Rye DB, Dihenia B, Weissman JD, Epstein CM, Bliwise DL. Presentation of narcolepsy after 40. Neurology 1998; 50(2): 459-465.
- American Academy of Sleep Medicine. International classification of sleep disorders: diagnostic and coding manual, 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.
- Attarian H. Chapter 6 narcolepsy in the older adult. In: Goswami M, Pandi-Perumal SS, Thorpy MJ, editors. Narcolepsy: a clinical guide, Humana Press; 2010. p. 69-76.
- Dauvilliers Y, Gosselin A, Paquet J, Touchon J, Billiard M, Montplaisir J. Effect of age on MSLT results in patients with narcolepsy-cataplexy. Neurology 2004; 62(1): 46-50.
- Olson LG, Cole MF, Ambrogetti A. Correlations among Epworth Sleepiness Scale scores, multiple sleep latency tests and psychological symptoms. J Sleep Res 1998; 7(4): 248-53.
Carlucci M, Prasad B. An 84-year-old woman with long-standing excessive daytime sleepiness. Ann Am Thorac Soc 2013;10:400–402.


