Contributed by Authors: Vinod Aiyappan, Laura Jarema, Nick Antic Institution: Adelaide Institute for Sleep Health (AISH), Repatriation General Hospital, Daw Park, Adelaide, South Australia, Australia
Question:
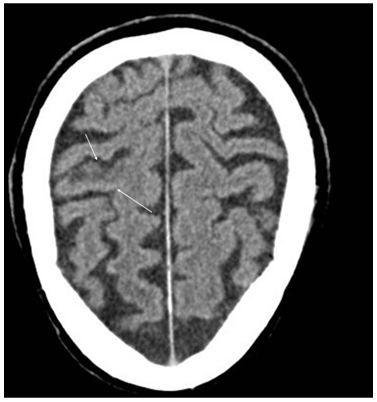
A 71-year-old man was admitted to the hospital with acute myocardial infarction which resulted in significant cardiac dysfunction. He also developed atrial fibrillation during this period, for which he was anticoagulated with warfarin. During the period of recovery (7 days after admission), he suffered a right hemispherical stroke with associated left hemiparesis (Figure 1).
Figure 1: CT scan showing cortical and subcortical low-density in the right pre-central gyrus (arrows)
He made a good recovery and was subsequently admitted to the rehabilitation ward for further management. During this time a ward-based diagnostic polysomnogram (PSG) was conducted as the patient reported excessive daytime sleepiness and the medical staff noted an abnormal breathing pattern. The PSG showed the following abnormalities.
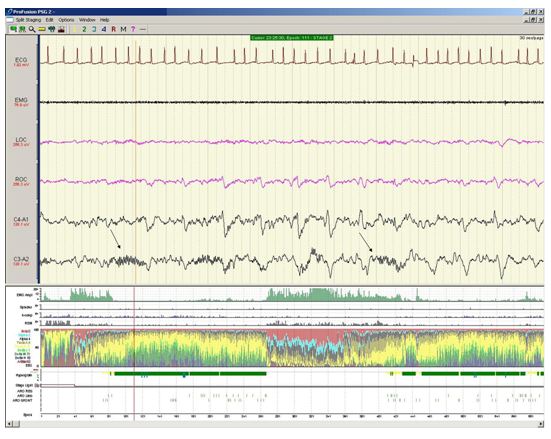
Figure 2:
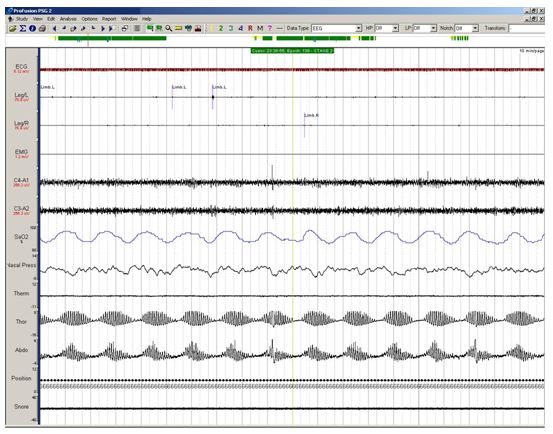
Figure 3:
1. What is the sleep-disordered breathing pattern (Figure 2), recorded during the PSG?
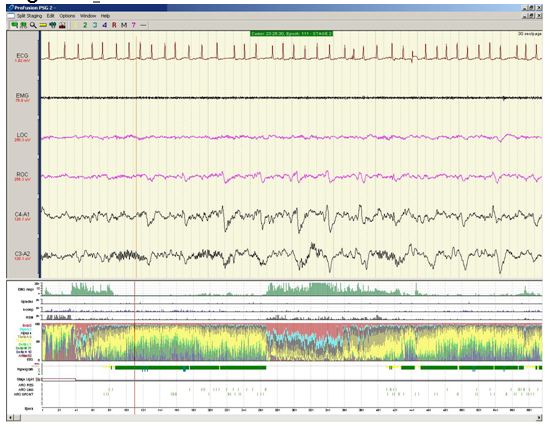
2. What is the abnormality noted in the C4-A1, EEG tracing (Figure 3)?
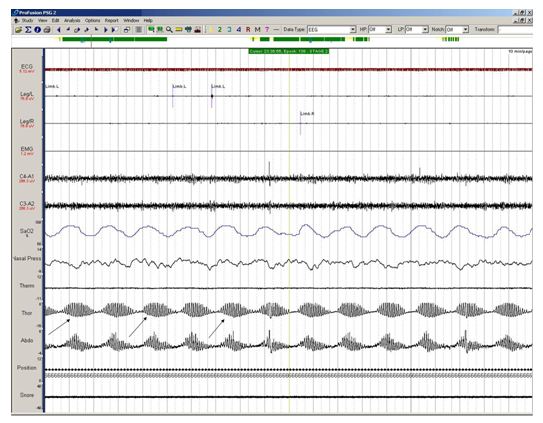
1. The sleep-disordered breathing documented is the classical Cheyne-Stokes respiration (CSR) characterised by cyclical crescendo-decrescendo pattern of breathing (see arrows in Figure 2 below) interspersed with central apneas and is predominantly seen in patients with congestive heart failure (please note that the nasal pressure channel was dislodged in this ward-based PSG, but the crescendo-decrescendo pattern of respiratory effort is clearly seen on the thoracic and abdominal effort bands). The patient was managed with optimization of his heart failure treatment and a CPAP trial was initiated. CPAP did not adequately control the oxygen desaturation and this was changed to Adaptive Servo- Ventilation (ASV) with good effect.
(Figure 2 with arrows)
2. The EEG shows a differential reduction in sleep spindles on the right sided EEG leads (C4-A1) compared to the left sided EEG (C3-A2) (see arrows in Figure 3 below). The CT scan of the head did not show any evidence of thalamic involvement, with the right sided stroke. A reduction in sleep spindles on the ipsilateral side of hemispherical cortical stroke has been reported and this has been thought to indicate that cerebral hemispheres play a major role in generation of synchronous sleep spindles.
(Figure 3 with arrows)
Discussion:
Sleep spindles are a distinctive feature that heralds the beginning of Stage II NREM sleep. The thalamus and corticothalamic structures are thought to be the main neuroanatomical structures that are responsible for spindle generation1. Corticothalamic projections are believed to be responsible for global coherence of sleep spindle oscillations. The functionality of the sleep spindle is still unclear but it is thought that sleep spindle oscillations block the flow of sensory information to cortex thereby promoting sleep continuity. They are also thought to be important in regulation of neuronal plasticity and memory consolidation2. Studies have shown that there is a reduction in sleep spindle frequency ipsilateral to the lesion in patients with stroke or other pathological processes1,2. In spectral analysis, Gottselig et al. also demonstrated that in patients who have had a hemispheric stroke there is reduction in size and coherence (this is a correlation measurement in the frequency domain) of sleep spindle activity ipsilateral to the lesion. This signifies the importance of cerebral hemispheres in generation of synchronous sleep spindles. They also observed an increase in the size and coherence of sleep spindle frequency, during the recovery stages of stroke.
CSR was first described by Dr. John Cheyne (1818), in a patient who suffered from congestive heart failure (CHF) and stroke4. CSR is characterised by crescendo-decrescendo pattern of breathing interspersed with periods of apnea which occur in a cyclical pattern. The prevalence of CSR has been estimated to be 20-40%, in patients with CHF and 6-28% in patients with stroke3. In patients with stroke the predisposing factors for CSR include left ventricular dysfunction, hypocapnia and enhanced central and peripheral chemosensitivity3. A key component in the management of CSR is optimization of heart failure treatment. CPAP therapy has been shown to be beneficial in some patients with CSR and congestive cardiac failure. Although the CANPAP trial failed to show any survival advantage in patients with heart failure on CPAP, subsequent post-hoc analysis showed an improved survival in those in whom CPAP reduced AHI to < 15 events/hr6. However in the CANPAP trial, CPAP treatment reduced the AHI in patients with CSR by only about 50%. Adaptive servo-ventilation (ASV) is a relatively new option in the treatment of CSR. These machines have an algorithm to analyse patients breathing pattern and alter the pressure support accordingly. ASV has been shown to improve AHI, left ventricular ejection fraction, pro-BNP levels and cardiopulmonary exercise test parameters, in patients with CHF, when added on to optimal anti-failure therapy5.
Our case report highlights two important PSG findings in a single patient.
References:
- De Gennaro L, Ferrara M. Sleep spindles: an overview. Sleep Medicine Reviews. 2003; 7(5):423-40.
- Gottselig JM, Bassetti CL, Achermann P. Power and coherence of sleep spindle frequency activity following hemispherical stroke. Brain. 2002; 125:373-383.
- Nopmaneejumrulsers C, Kaneko Y, Hajek V, Zivanovic V, Bradley TD. CSR in stroke. Am J Resp Crit Care Med. 2005; 171:1048-1052.
- Cheyne J. A case of apoplexy in which the fleshy part of the heart was converted into fat. Dublin Hospital Reports. 1818; 2:216–23.
- Oldenburg O et al. ASV improves cardiac function in patients with chronic heart failure and Cheyne - Stokes respiration. Eur. Journal of Heart Failure. 2008; 10:581-586.
- Bradley TD, Logan AG, Kimoff RJ, Series F, Morrison D, Ferguson K, Belenkie I, Pfeifer M, Fleetham J, Hanly P, Smilovitch M, Tomlinson G, Floras JS, for the CANPAP Investigators. Continuous positive airway pressure for central sleep apnoea and heart failure. N Engl J Med. 2005; 353:2025–2033.


