Contributed by Martin A Glasser, Joerg Steier and Mary J Morrell. NHLI, Imperial College London and NIHR Respiratory BRU at The Royal Brompton and Harefield NHS Trust.
A 51 year old lady presented with an 18 month history of excessive daytime sleepiness (Epworth Sleepiness Scale 16/24), snoring and morning headaches. She had no history of pulmonary disease. Her height was 158cm and she weighed 136kg (body mass index—BMI— 54.5kg/m2). Respiratory and cardiovascular examinations were unremarkable, but resting daytime blood gases breathing room air revealed a PaCO2 of 6.7 kPa (50.4 mmHg) and PaO2 of 8.8 kPa (66.2 mmHg). PH was 7.38. Her spirometry results were: FEV1 1.55 l (61% predicted), FVC 2.03 l (68% predicted), FEV1/FVC 76%.
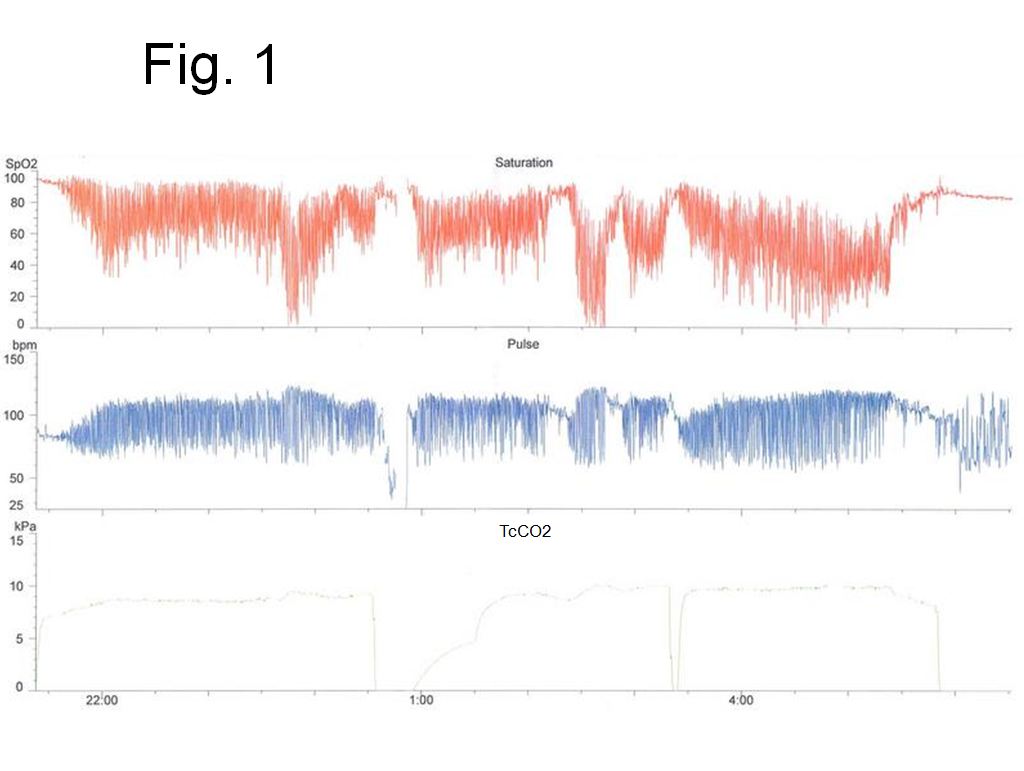
She was admitted electively for nocturnal O2 / CO2 monitoring (Fig. 1).
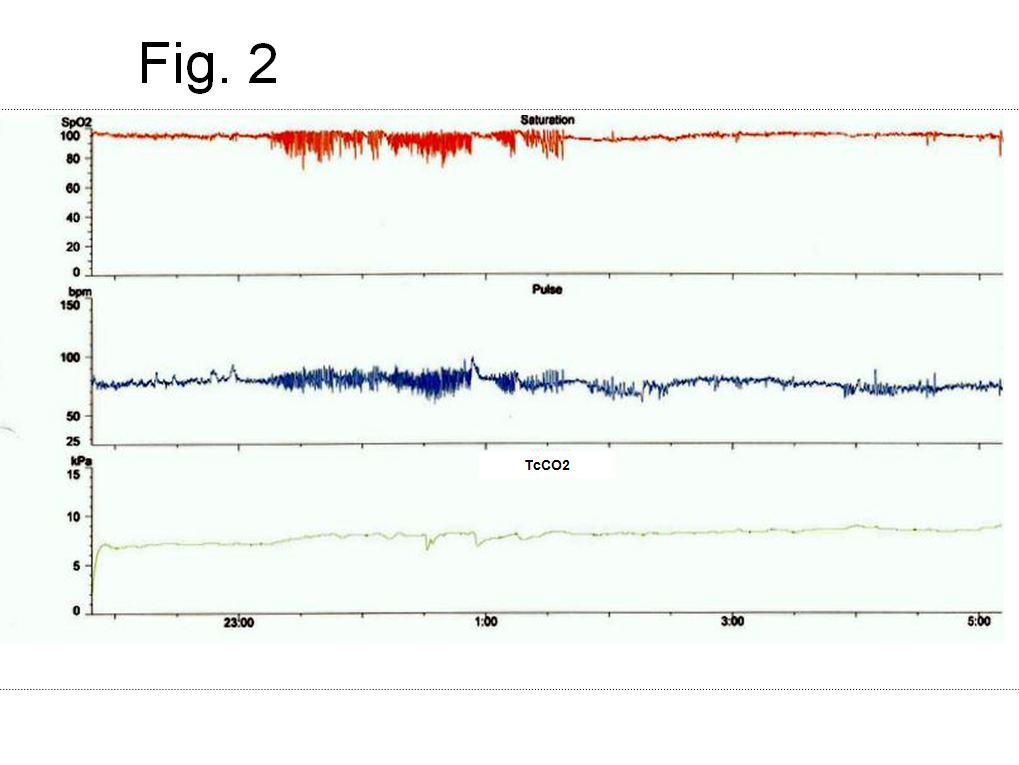
On the second night of her admission, an intervention was made and O2 / CO2 monitoring was repeated (Fig. 2).
-
What was the diagnosis?
-
What was the intervention?
Answers:
-
The patient is morbidly obese, with a BMI of 54 kg/m2. Her O2 / CO2 monitoring on admission (Fig. 1) shows evidence of severe sleep disordered breathing and profound nocturnal hypoventilation, with mean overnight oxygen saturations of 70% and mean TcCO2 of 8.6 kPa (64.7 mmHg). Time with TcCO2 above 6 kPa (45 mmHg) was 7 hours 20 minutes. She remains hypercapnic throughout the day and her spirometry suggests a restrictive process. These features are the hallmarks of obesity hypoventilation syndrome (OHS).
-
The introduction of non-invasive ventilation (NIV) (Inspiratory positive airway pressure [IPAP] 18 cmH2O, expiratory airway pressure [EPAP] 4 cmH2O) produced a marked reduction in both frequency and magnitude of oxygen desaturations (mean SaO2 93%) and a reduction in transcutaneous CO2 (mean TcCO2 7.8 kPa, 58.6 mmHg) (Fig. 2). However, there was still evidence of significant hypoventilation, with 7 hours and 19 minutes spent with TcCO2 above 6 kPa (45 mmHg). Furthermore, her PaCO2 was 8.28 kPa (62.3 mmHg) on an early morning room air arterial blood gas. The following night, IPAP was increased to 21 cmH2O and EPAP to 7 cmH2O, in order to further improve ventilation and eliminate upper airway obstruction. On an early morning arterial blood gas her PaCO2 was found to be 7.58 kPa (57mmHg) and her IPAP was further increased to 23 cmH2O. On a subsequent morning arterial blood gas her PaCO2 was 7.51 kPa (56.5 mmHg). Although this implies that there is ongoing nocturnal hypoventilation, this had markedly improved from admission. Therefore, the patient was discharged home that day, with an increased IPAP of 25 cmH2O, with a plan to reassess her ventilatory status in clinic. No supplemental oxygen was given at any stage.
Discussion
Obesity Hypoventilation Syndrome (OHS), the co-existence of obesity (BMI > 30 kg/cm2) and daytime hypercapnia, in the absence of another cause of hypoventilation, affects approximately 1 in 300 people. It is classified by ICSD as a sleep related hypoventilation / hypoxemia due to a chest wall disorder. The prevalence of OHS is likely to rise as a result of the global obesity epidemic1. The 18-month mortality in OHS patients discharged from hospital is 2.5 times higher than that in obese patients without OHS. OHS is also associated with increased rates of hypertension, angina, peripheral oedema, pulmonary hypertension and cor-pulmonale2.
Pathophysiology of OHS: Deposition of fat, around the abdomen and thorax results in increased work of breathing. Lung volumes, especially vital capacity and expiratory reserve volume are greatly reduced, which reduces chest wall compliance and increases airway resistance. The work of breathing is further increased by expiratory flow limitation caused by gas trapping in small airways as a result of breathing at reduced lung volumes. This is exacerbated when supine3.
Many obese subjects are able to maintain their minute ventilation by increasing respiratory rate. It has been hypothesised that, in OHS patients, transient hypercapnia as a result of apnoeas induced by sleep disordered breathing may trigger a mechanism that leads to hypoventilation and hypercapnia even during the day. Nocturnal acidaemia, as a consequence of hypercapnia, results in an increased rate of bicarbonate reabsorption in the kidneys. This increased bicarbonate concentration may blunt the ventilatory drive induced by hypercapnia and lead to daytime hypoventilation4. It has also been shown that central fat deposition is increased in OHS patients compared to eucapnic obese subjects, as evidenced by larger neck circumferences and higher waist to hip ratios5.
A further mechanism for depression of ventilatory drive in OHS is leptin resistance. Leptin is a polypeptide produced by adipose tissue, which acts on satiety centres in the hypothalamus to suppress hunger. Leptin is also a respiratory stimulant. In humans, obesity is a leptin resistant state. Thus, although obese subjects have elevated leptin concentrations, this may not produce a corresponding increase in ventilatory drive6.
Management of OHS: Weight loss reverses many of the effects of obesity on the respiratory system. However, for morbidly obese subjects, this is often difficult to achieve and even more difficult to maintain. A multidisciplinary approach is required with the provision of psychological support, detailed dietetic and exercise plans, and input from endocrinologists, chest physicians and bariatric surgeons. Bariatric surgery has been shown to improve lung volumes, gas exchange and parameters of sleep disordered breathing in obese subjects7. However bariatric surgery is inadequate as the sole therapy for OHS. The AHI remains elevated after surgery and weight loss is often only temporary8.
Nocturnal non-invasive ventilation (NIV) is also important in the management of OHS, both as an adjunct to weight loss and in those patients in whom weight loss has not been achieved. NIV improves daytime sleepiness and PaCO2 in OHS. It is also associated with improved quality of life and a reduction in hospital admissions. OHS patients who refuse NIV have a significantly higher mortality than those who accept it9. Continuous positive airway pressure may also be effective in reducing sleepiness and PaCO2 in up to 80% of OHS patients. However, there is only limited evidence of its effects on prognosis10.
References:
1. Mokhlesi B. Obesity hypoventilation syndrome: a state of the art review. Respir Care. 2010 Oct;55(10):1347-62.
2. Kessler R, Chaouat A, Schinkewitch P, Faller M, Casel S, Krieger J, Weitzenblum E. The obesity-hypoventilation syndrome revisited: A prospective study of 34 consecutive cases. Chest 2001;120:369-376.
3. Pankow W, Podszus T, Gutheil T, Penzel T, Peter J, Von Wichert P. Expiratory flow limitation and intrinsic positive end-expiratory pressure in obesity. J Appl Physiol 1998;85:1236-1243.
4. Berger KI, Goldring RM, Rapoport DM. Obesity hypoventilation syndrome. Semin Respir Crit Care Med 2009;30:253-261.
5. Resta O, Foschino-Barbaro MP, Bonfitto P, Talamo S, Legari G, De Pergola G, Minenna A, Giorgino R. Prevalence and mechanisms of diurnal hypercapnia in a sample of morbidly obese subjects with obstructive sleep apnea. Respir Med 2000;94:240-246.
6. Campo A, Fruhbeck G, Zulueta JJ, Iriarte J, Seijo LM, Alcaide AB, Galdiz JB, Salvador J. Hyperleptinemia, respiratory drive and hypercapnic response in obese patients. Eur Respir J 2007;30:223-231.
7. Thomas PS, Cowen ER, Hulands G, Milledge JS. Respiratory function in the morbidly obese before and after weight loss. Thorax 1989;44: 382-386.
8. Piper AJ, Grunstein RR. Obesity hypoventilation syndrome: mechanisms and management. Am J Respir Crit Care Med. 2011 Feb 1;183(3):292-8.
9. Berg G, Delaive K, Manfreda J, Walld R, Kryger MH. The use of health-care resources in obesity-hypoventilation syndrome. Chest 2001;120:377-383.
10. Piper AJ, Wang D, Yee BJ, Barnes DJ, Grunstein RR. Randomised trial of CPAP vs bilevel support in the treatment of obesity hypoventilation syndrome without severe nocturnal desaturation. Thorax 2008;63(5):395-401.


