Not Enough
Siddharth Dugar, MD
Critical Care Fellow, Cleveland Clinic, OH
Robert L. Chatburn, MHHS, RRT-NPN, FAARC
Professor, Department of Medicine, Lerner College of Medicine of Case Western Reserve University
Consider a 34 year old male with a history of portal hypertension presented with fever, change in mental status and hypotension. The patient was intubated for airway protection.
The current ventilator settings are Volume Controlled-Continuous Mandatory ventilation (VC-CMV) mode with RR 18/min, tidal volume of 460ml, a flow rate of 70L/min with a decelerating flow waveform and PEEP of 5cm H2O and FiO2 of 40%.
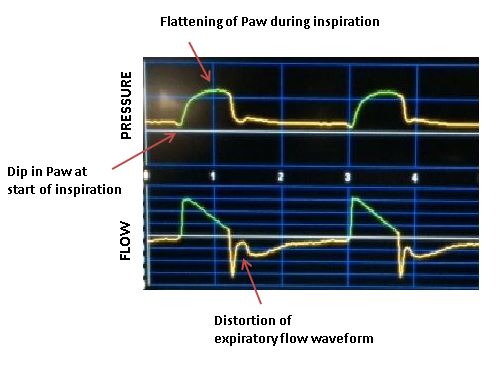
You observe the following flow and pressure waveforms (Figure 1):
Figure 1. Observed waveform showing signs of asynchrony
What form of patient ventilator asynchrony is clearly evident?
- Delayed inspiratory cycling
- Premature cycling
- Ineffective Triggering.
- Auto Triggering.
Answer 2 Premature cycling
To interpret this waveform, we need to know what an ideal waveform would look like for a passive patient given the equation of motion:
Pvent + Pmus = (elastance x volume) + (resistance x flow)
Where Pvent = pressure generated by the ventilator and Pmus is pressure generated by the ventilatory muscles (zero for a paralyzed patient). Any deviations from the expected ideal can be evidence of asynchrony. For a passive patient in this mode of ventilation we would expect to see the waveform shown in Figure 2.
Figure 2. Idealized waveforms for VC with descending ramp flow

During inspiration with this flow waveform the initial rise in Paw is due to airway resistance, with no component due to elastance x volume because volume is still zero. As volume accumulates, Paw increases but the component due to elastance x volume becomes larger relative to the component due to resistance x flow because flow is decreasing. At the end of inspiration, Paw is lower than the peak value (at mid inspiration) because flow has dropped to zero. Of course, the actual shape of the Paw curve depends on the relative values of resistance and elastance. But for patients with stiff lungs, there is generally a hump in the pressure waveform.
During exhalation, peak expiratory flow is simply (elastance x volume)/resistance. Flow then decays according to the time constant (resistance/elastance or resistance x compliance). Thereafter flow decreases exponentially to zero, flow waveform depending on product of resistance and compliance also known as “time constant”.
Given this understanding of the ideal waveforms for a passive patient, we can now interpret the actual waveform. First, we recall that for volume control modes, the right hand side of the equation of motion must remain unchanged in the face of active inspiration (Pmus greater than zero) because the tidal volume and flow are preset (and we assume elastance and resistance are constant). Hence, active inspiration must deform the Paw waveform (i.e., as Pmus increases, Pvent decreases)
Now, we see that Paw dips just prior to the start of inspiratory flow. This indicates patient triggering and thus the presence of Pmus (i.e., active inspiration). Next we see a flattening of Paw during inspiration compared to the expected passive waveform. Again, this indicates active inspiration. When the ventilator cycles inspiration off, there is an immediate drop in the total applied pressure because Pvent goes to zero. As a result there is a short spike in expiratory flow. However, flow does not decay smoothly as expected for a passive exhalation. Rather, the flow waveform is distorted toward zero. This implies a force in the inspiratory direction, which can only be due to Pmus. Indeed, we can fairly conclude that Pmus continues even though Pvent stops. Hence, the “neural inspiratory time”, or the duration of Pmus controlled by the brain, is longer than the set inspiratory time, which is determined by the preset tidal volume and inspiratory flow. Hence, we conclude that the asynchrony we see can be classified as premature cycling.
In summary, premature cycling arises when the ventilator terminates the breath but the inspiratory muscles continue to contract from patient effort; as the inspiratory time set on ventilator is shorter than the neural inspiratory time of the patient. If the patient continues to generate inspiratory muscle pressure during expiration, this expiratory flow pattern may be affected in one of the following ways.
- Inspiratory (positive) flow for some time after opening of the exhalation valve followed by peak expiratory flow
- A sharp decrease from the peak expiratory flow which lasts a few milliseconds followed by an increase and then decreases gradually to zero toward the end of expiration (as seen in our patient).
- A sharp decrease from the peak expiratory flow to positive flow causing mechanical ventilator to sense a second effort, resulting in a second breath causing stacking of breaths, also known as “double triggering.”
The phenomenon seen in our patient is from the elastic recoil pressure being higher at end-inspiration than inspiratory muscle creating an expiratory flow. As volume decreases, the elastic recoil pressure declines; while inspiratory muscles continue to contract increasing opposing pressure to expiratory flow causing a corresponding decrease in expiratory flow. Relaxation of inspiratory muscles eliminates this opposing pressure and expiratory flow increases.
The most convincing way to confirm patient effort is with a Pes (Esophageal pressure) or Edi signal (electrical activity of the diaphragm) but clinical application of such invasive procedure is limited.
The flow and pressure waveform can be used to determine patient effort. The dip in the pressure waveform before the start of inspiration seems to indicate that inspiration was patient triggered. Also there is small hump in Paw, possibly indicating that Paw was decreased by an increase in Pmus, again indicating inspiratory effort throughout the preset inspiratory time and hence the classification of premature cycling.
REFERENCE:
- Gentile MA. Cycling of the mechanical ventilator breath. Respir Care. 2011 Jan;56(1):52-60.
- Nilsestuen JO, Hargett KD. Using ventilator graphics to identify patient-ventilator asynchrony. Respir Care. 2005 Feb;50(2):202-34.


