Fire in the Chest
Shambo Guha Roy1, MD, Oleg Kinaschuk2, MD, Candace Griffith2, MD, Fatima Babar2, MD
1 Department of Radiology, Mercy Catholic Medical Centre, Darby, PA
2 Department of Medicine, Mercy Catholic Medical Centre, Darby, PA
Case
A 45-year-old male with a history of HIV for 20 years, IV drug use, hypertension, asthma and questionable medication adherence presented to the ED with progressively worsening shortness of breath over the past month, new-onset fevers and bloody stools. His home medication regimen consisted of abacavir, dolutegravir, lamivudine, azithromycin, trimethoprim-sulfamethoxazole, amlodipine and lisinopril.
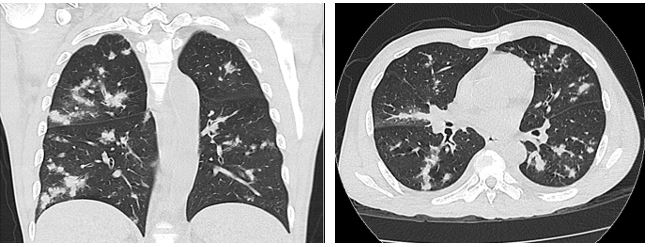
On admission, he was febrile (103.8°F), tachycardic and tachypneic. Physical exam revealed extensive purple-pink skin lesions and lower extremity pitting edema with no clinical signs of cellulitis. Lymph node exam was significant for supraclavicular, axillary, and inguinal lymphadenopathy. Labs revealed hemoglobin of 5.3 g/dl, lactate of 3.5 mmol/L and absolute CD4 count of 19 cell/ul. CT scans of the chest, abdomen and pelvis revealed multiple retroperitoneal and mesenteric lymph nodes, as well as multiple lytic lesions involving the pelvis and thoracolumbar vertebrae. Representative images from the chest CT are shown below:
Images 1 & 2
Question
What is the diagnosis?
- Multifocal Bacterial Pneumonia
- Pulmonary Aspergillosis
- Tuberculosis
- Kaposi Sarcoma
- Lymphoma
- Pneumocystis Pneumonia
D. Kaposi Sarcoma
Discussion
Kaposi sarcoma (KS) is a low-grade spindle cell tumor derived from the endothelium, most commonly associated with Human Herpes Virus-8 infection [1]. There are four clinical and epidemiological variants of the disease: classic (sporadic or Mediterranean), endemic (African), iatrogenic (organ transplant–related), and AIDS–related (epidemic) KS [2]. It is the most common solid tumor in HIV patients with an overall incidence of 481 per 100,000 person-years [3].
Disseminated KS can involve any organ, the most common of which include skin, lymph nodes, lung, GI tract, liver and spleen. Pulmonary KS can have a variety of presentations, with variable involvement of the lung parenchyma, mediastinum and pleura. The classic presentation is the presence of bilateral symmetric ill-defined 'flame shaped' nodules in a peribronchovascular distribution. The nodules are usually greater than a centimeter and frequently surrounded by ground glass opacities giving a “halo’ appearance. Other less common findings include asymmetrically distributed nodules and larger masses [4]. Peribronchovascular and interlobular septal thickening are commonly encountered, often associated with mediastinal and axillary lymphadenopathy. Pleural disease is often associated with bilateral pleural effusions. Less commonly, fissural nodularity and bilateral pleural implants are seen.
Our patient showed classic radiological picture of pulmonary KS. He had biopsies of both skin and lymph nodes confirming KS. Due to the classic radiological appearance and histopathological evidence from two other sites, a lung biopsy was not performed. He was scheduled to receive chemotherapy with doxorubicin [5].
References
-
Chang Y, Cesarman E, Pessin MS, et al. Identification of herpesvirus-like DNA sequences in AIDS-associated Kaposi’s sarcoma. Science 1994; 266: 1865–9.
-
Tappero JW, Conant MA, Wolfe SF, et. al. Kaposi’s sarcoma: epidemiology, pathogenesis, histology, clinical spectrum, staging criteria and therapy. J Am AcadDermatol 1993; 28: 371–95.
-
Liu Z, Fang Q, Zuo J, et. al. The world-wide incidence of Kaposi's sarcoma in the HIV/AIDS era. HIV Med 2018; 19(5): 355-64.
-
Restrepo CS, Martínez S, Lemos JA, et. al. Imaging manifestations of Kaposi sarcoma. Radiographics 2006; 26(4): 1169-85.
-
Northfelt DW, Dezube BJ, Thommes JA, et. al. Pegylated-liposomal doxorubicin versus doxorubicin, bleomycin, and vincristine in the treatment of AIDS-related Kaposi's sarcoma: results of a randomized phase III clinical trial. J ClinOncol 1998; 16(7): 2445-51.


