Endobronchial Ultrasound: beyond tumors and lymph nodes
Ghassan Kamel, Armin Krvavac, Pujan H Patel, Christopher Barrios, David Stoeckel
Division of Pulmonary, Critical Care and Sleep Medicine, Department of Internal Medicine,
Saint Louis University School of Medicine, Saint Louis, MO
Case
A 57-year-old female with a history of rheumatoid arthritis on chronic prednisone and methotrexate was admitted to the hospital with acute hypoxic respiratory failure. She was initially admitted to the medical intensive care unit (ICU) with a diagnosis of pneumonia but she did not improve with antibiotics. Given her risk factors for opportunistic infections, a diagnostic bronchoscopy with linear endobronchial ultrasound (EBUS) was performed. An abnormality in the pulmonary artery was noted (Figure 1).
Figure 1:
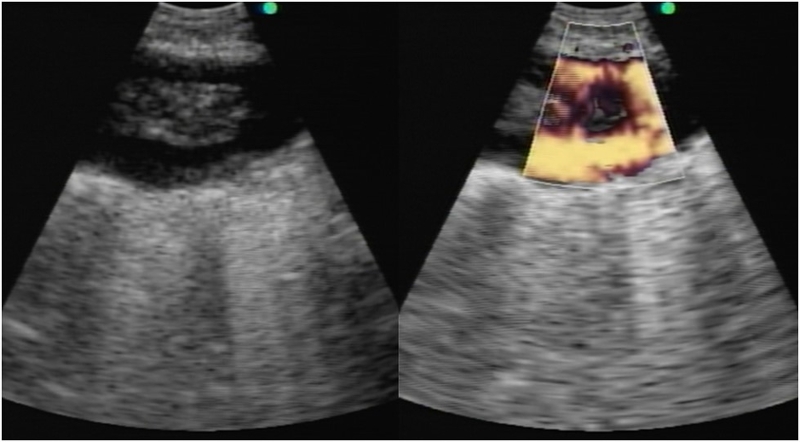
Question: What is the abnormality observed in the images above?
There is a filling defect in the pulmonary artery, which most likely represents a pulmonary embolism (PE).
Discussion:
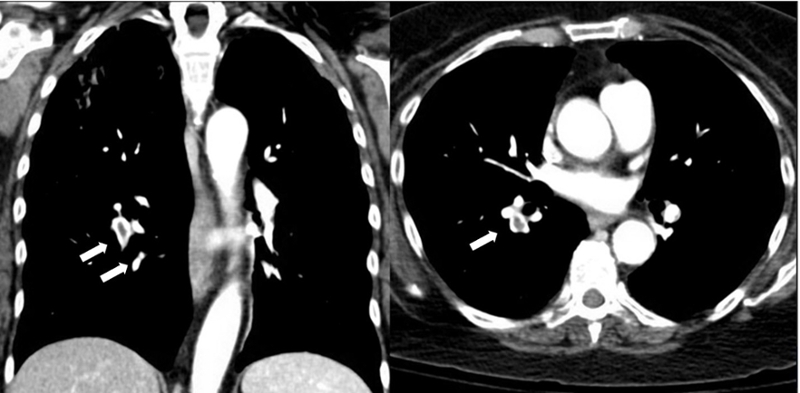
Linear EBUS examination of the pulmonary artery revealed a large echogenic lesion with flow around it on doppler consistent with pulmonary embolism. A lower extremity ultrasound revealed a deep vein thrombosis for which she was started on therapeutic anticoagulation. A CT angiogram was not performed as it would not have altered the management of the patient. A few days later, she was readmitted for a gastrointestinal hemorrhage. During that second hospitalization, the patient had CT scan of the chest that confirmed the diagnosis of bilateral pulmonary emboli (Figure 2).
Figure 2:
Linear EBUS has been reported in the literature to detect incidental central pulmonary emboli [1-4] with an accuracy of more than 95% in patients undergoing the procedure for lung cancer staging [2]. CT angiography remains the preferred modality to diagnose PE [5]. However, for patients with renal failure, contrast allergy, or clinical instability precluding travel out of the ICU, linear EBUS may be considered to detect central PE. The routine use of EBUS to diagnose PE is not recommended but pulmonologists performing EBUS for other reasons should be aware of this possible finding.
References:
-
Sachdeva A, Lee HJ, Malhotra R, Shepherd RW. Endobronchial ultrasound diagnosis of pulmonary embolism. J Bronchol Intervent Pulmonol 201;:20:33-34.
-
Aumiller J, Herth FJF, Krasnik M, et al. Endobronchial ultrasound for detecting central pulmonary emboli: a pilot study. Respiration. 2009;77:298–302
-
Segraves JM, Daniels CE. Pulmonary embolus diagnosed by endobronchial ultrasound. Respir Med Case Rep 2015;16:104.
-
Dhillon SS, Harris K. Endobronchial ultrasound for the detection of chronic pulmonary artery thrombus. Endoscopic Ultrasound. 2016;5(4):272-273.
-
Fedullo PF, Tapson VF: The evaluation of suspected pulmonary embolism. N Engl J Med 2007;349:1247–1256


