Dyspnea and Recurrent Urinary Tract Infections
Max Martin, M.D.1, Kelly Pennington, M.D.2, Jay H. Ryu M.D.2
1Division of General Internal Medicine and 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Mayo Clinic, Rochester, MN
Case
A 31-year-old female nurse presents with a 4-month history of progressive, exertional dyspnea. Her only associated symptoms are mild, nonproductive cough. She denies fevers, chills, weight loss, joint pains, odor sensitivity, seasonal variation, or skin changes. She previously smoked for about 1 year in her early 20s. She denies any relevant environmental exposures including molds, birds and hot-tubs. She has no family history of pulmonary disease including asthma.
Her medical history is notable only for endometriosis requiring laparoscopic vaginal hysterectomy. Her postoperative course has been complicated by recurrent urinary tract infections requiring multiple treatments of antibiotics. For the last 6 months, she has been receiving a daily suppressive antibiotic.
On exam, she is afebrile and hemodynamically stable. She is in no distress. Her cardiac exam is unremarkable. Her lungs are clear to auscultation. She has no rashes or synovitis of the large or small joints.
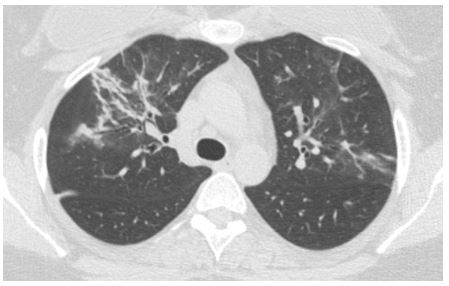
Complete pulmonary function tests are normal. Chest x-ray demonstrates bilateral, patchy opacities prompting further imaging. Representative images from her high-resolution chest CT is shown below:
Question
What additional information is most likely to provide the diagnosis?
- Bronchoscopy with bronchoalveolar lavage
- Extractable nuclear antigen antibody panel
- Methacholine challenge test
- Review of medication list
D. Review of medication list
Discussion
High resolution CT chest revealed patchy consolidative and ground-glass opacities more prominent in the upper lobes, right greater than left.
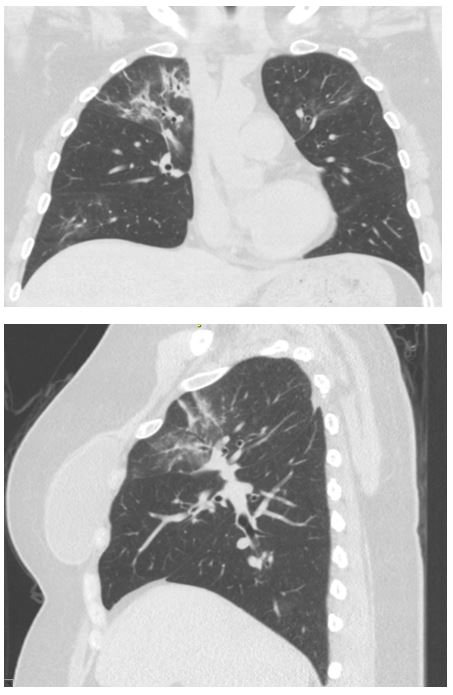
The most likely diagnosis based on the clinical context, presentation, and radiographic findings is chronic nitrofurantoin-induced lung toxicity. Nitrofurantoin was discontinued with resolution of her respiratory symptoms. Repeat CT chest 3 months later (shown below) demonstrated complete resolution of the irregular consolidative opacities.

Nitrofurantoin-induced lung toxicity has two different presentations: acute hypersensitivity or sub-acute to chronic pneumonitis [1]. The exact pathogenesis is unclear, but the acute reaction most resembles a hypersensitivity reaction [1], while the chronic reaction has features of a cell-medicated and/or toxic response [2, 4]. Acute nitrofurantoin hypersensitivity occurs within 2 weeks of the initial exposure. Symptoms include fever, dyspnea, and cough. Sub-acute to chronic nitrofurantoin pneumonitis is insidious in onset and develops over several months [2]. It often occurs in patients who are on chronic suppressive therapy, and manifests as progressive dyspnea.
Nitrofurantoin-induced lung toxicity is diagnosed by establishing a temporal relationship between symptoms and drug exposure. Chest CT usually reveals patchy areas of consolidation with a ‘streaky’ appearance consistent with organizing pneumonia pattern [2]. PFTs can either be normal or display a restrictive pattern, with the latter being more common in the chronic presentation.
Treatment of nitrofurantoin-induced lung toxicity is cessation of the offending medication. For patients with acute hypersensitivity, regression of symptoms and resolution of radiographic abnormalities occurs over days to weeks. For sub-acute/chronic pneumonitis, symptoms and radiographic changes resolve over weeks to months [2, 3]. The incidence of residual infiltrates and symptoms is higher with the chronic pneumonitis [2, 4]. Some physicians have utilized oral glucocorticoids as a treatment option, although there is no strong evidence to support this. Use of glucocorticoids should be individualized, but may be beneficial the setting of extensive pulmonary infiltrates associated with pronounced respiratory symptoms or pulmonary dysfunction. There is a high rate of recurrence associated with repeat exposure, so further use of nitrofurantoin should be strictly avoided.
References
-
Mendez JL, Nadrous HF, Hartman TE, Ryu JH. Chronic nitrofurantoin-induced lung disease. Mayo Clin Proc 2005; 80: 1298-302.
-
Rosenow EC, DeRemee RA, Dines DE. Chronic Nitrofurantoin Pulmonary Reaction. NEJM 1968; 279: 1258-1262.


