Case of the curious opacification
Janaki Deepak, MBBS, FACP
Assistant Professor, Pulmonary and Critical Care Medicine,
University Of Maryland School Of Medicine, Baltimore, MD
Case:
A 57 year old male with hypertension and hyperlipidemia presented with vague discomfort in the chest, shortness of breath and malaise for a few weeks. He denied any cough, fever, orthopnea, or palpitations. He has had decreased appetite and 5 pound weight loss.
Social History: Smoker, 40 pack year smoking history. Denies alcohol or drug use. Some exposure to asbestos in his early 20s.
Physical exam: T: 36.5, P: 98, BP: 110/67, RR: 20, 95% on room air
General: Obese male in minimal distress. Lungs: Decreased breath sounds on the left upper zone, no egophony, no dullness to percussion.
Heart: S1, S2 normal no murmurs, rubs, gallop
Basic labs and EKG are normal.
Chest x-ray:
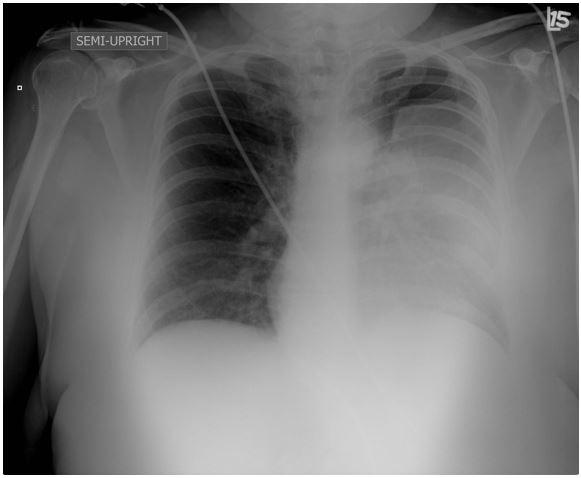
Based on the Chest x-ray above what would be the next best step in management of this patient?
- Admit the patient and start on antibiotics for community acquired pneumonia
- Perform an ultrasound guided thoracentesis
- Obtain a CT and plan for a bronchoscopy for tissue biopsy
- Inform the patient that his x-ray only shows an artifact (skin fold mimicking haziness) and discharge home.
Correct Answer 3
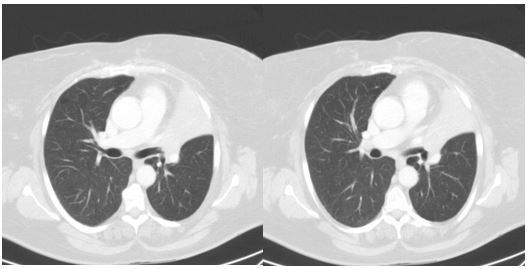
The Chest x-ray shows left upper lobe collapse due to an endobronchial squamous cell lung cancer. CT shown below:
Chest X-ray signs of left upper lobe collapse:
-
In many cases of left upper lobe collapse, the anterior parts of the aortic arch and the aortic knuckle are abutted by collapsed lung and thus the normal silhouette is lost.
-
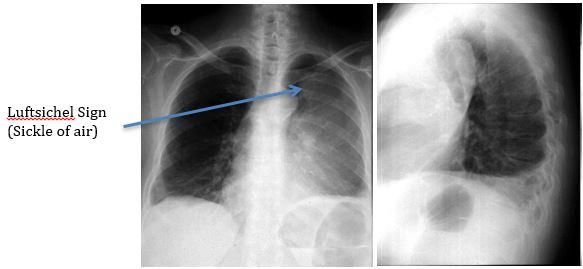
In some cases the apical (superior LB6) segment of the left lower lobe is hyperinflated and becomes interposed between the collapsed lung and the aortic arch. In such cases the aortic knuckle becomes visible and the collapsed left upper lobe is thus displaced laterally away from the mediastinum. This appearance of the air crescent around the aortic arch is called “Luftsichel” sign. It is derived from the German words luft = air, sichel = sickle.
-
The left upper lobe collapses anteriorly becoming a thin sheet of tissue apposed to the anterior chest wall. This appears as a hazy or veil-like opacity extending out from the hilum and fading out inferiorly; this often obscures the left heart border.
-
There is loss of volume of the left hemithorax with elevation of the left hemidiaphragm. However the left hemidiaphgram is still visible indicating that the left lower lobe is spared.
-
Peaked or tented hemidiaphgram called the “Juxtaphrenic peak sign”.
-
Other findings include: vascular splaying, hilar shifts, and shift of the major fissure anteriorly on lateral view.
Radiographic signs of Collapse:
Direct signs
- Displaced fissures
- Crowded bronchovascular markings
- Shifted position of a marker structure such as a scar, nodule, or granuloma
Indirect signs
- Shifts in the positions of the hila, diaphragm, and mediastinum
- Increased density or radio-opacity of the lung tissue
- Crowding of the ribs
- Loss of hemidiaphragm shadow
Another example of left upper lobe collapse
References:
- Donna G. Blankenbaker, MD , Signs in Radiology: Radioiogy 1998; 208:319-320
- Collins J, Stern EJ. Chest radiology, the essentials. Lippincott Williams & Wilkins. (2007) ISBN:0781763142.


