An embryonic cause of cough
Hasan S. Yamin, MD1, Yousef Abuasbeh, MD2
1 Pulmonary and Critical Care Department
An-Najah National University Hospital, Palestine.
2Thoracic Surgery Department
St. Joseph Hospital, Palestine
Case
A 53-year-old nonsmoking woman presented to pulmonary clinic with progressive dry cough of several years duration, associated with mild exertional dyspnea. Her past medical history is significant for well controlled diabetes mellitus and hypertension. She denied wheezing, chest pain, hemoptysis, anorexia, weight loss, occupational exposure or recent travel.
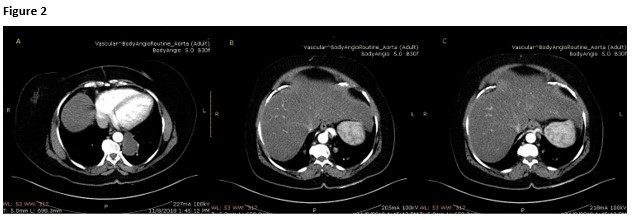
Routine labs were within normal limits. Her chest film and chest CT scan with IV contrast are shown below (Figure 1).

Question
What is the most likely diagnosis?
- Primary lung cancer
- Bilateral pneumonia
- Intralobar pulmonary sequestration
- Extralobar pulmonary sequestration
- Bronchogenic cysts
Answer C: Intralobar pulmonary sequestration
Discussion
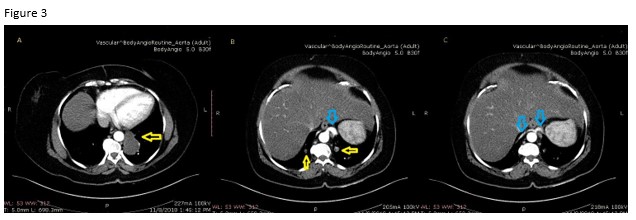
Chest CT scan with IV contrast showed bilateral lower lobe masses larger on the left, suggestive of lung sequestration (yellow arrows), which was confirmed on CT Aortogram (Figure 3). Sequestered lung lacks normal communication with the rest of tracheo-bronchial tree, and receives its arterial blood supply from the systemic circulation, while maintaining normal venous drainage to the left atrium. It is a rare congenital anomaly resulting from faulty embryogenesis of the tracheo-bronchial tree (1). Broncho pulmonary sequestrations are either extra lobar when they have separate pleural covering, or intralobar when they share pleura with rest of lung (2). This patient has bilateral intralobar pulmonary sequestrations with feeding arterial supply from descending thoracic aorta 5 mm on the right and 1.08 mm on the left (blue arrows).
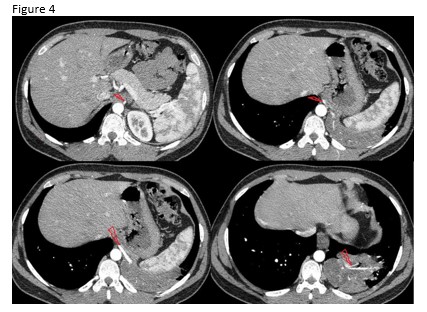
Primary lung cancer (A) is unlikely to be true as the patient`s symptoms have been going on for a few years, and patient denies symptoms like anorexia or weight loss. Pneumonia (B) would not have its own systemic blood supply. Extralobar sequestration (D) is also incorrect. Figure 4 shows an example of an extra lobar sequestration in the LLL with feeding vessels from aorta (Red arrows). Note that sequestered lung in this example shares same pleura with the rest of lung. Bronchogenic cysts (E) are also caused by abnormal branching of the tracheobronchial tree during embryogenesis. These fluid-filled structures are usually located in the mediastinum and rarely in the lungs. Although they do not communicate with rest of airways, they maintain their pulmonary blood supply (3).
References
-
Deepa RB, Teresa C, Mark RF, et. al. Congenital lung abnormalities: Embryologic features, prenatal diagnosis, and postnatal radiologic-pathologic correlation. RadioGraphics 2010; 30: 1721–38.
-
Yamin HS, Alastal AY. Pulmonary Sequestration Supplied by an Aberrant Infra-diaphragmatic Artery. J Pulm Respir Med 2017; 7: 3. doi: 10.4172/2161-105X.1000413
-
Baral D, Adhikari B, Zaccarini D, et. al. Congenital Pulmonary Airway Malformation in an Adult Male: A Case Report with Literature Review. Case Reports in Pulmonology 2015; 2015: 743452. doi: 10.1155/2015/743452.


