Acute Onset Shortness of Breath, Pleuritic Chest Pain, and Cough
Slostad, JA1, Higgins, AS1, Dempsey TM2, Dunn WF2
1Department of Internal Medicine, 2Department of Pulmonary and Critical Care Medicine
Mayo Clinic, Rochester, Minnesota, USA
Case
A 65-year-old non-smoking female presented to the emergency department with one week of dyspnea, pleuritic chest pain, and dry cough.
On exam, she was afebrile, hemodynamically stable with blood pressure 150/77, oxygen saturation of 92% on room air, and respiratory rate of 22. She had shallow work of breathing with right-sided absent breath sounds in the mid and lower lung base. She had several white dome-shaped papules scattered over her forehead and face. Cardiac, neurologic, and abdominal exams were unremarkable. Family history was significant for a brother with tension pneumothorax requiring pleurectomy. Chest x-ray was obtained (Figure 1).
Figure 1: Chest x-ray obtained in Emergency Department:

Question
What is the most likely cause of her acute onset of shortness of breath, pleuritic chest pain, and dry cough?
- Malignant pleural effusion
- Primary pneumothorax
- Secondary pneumothorax with tension physiology
- COPD exacerbation
- Community acquired pneumonia
Answers: C. Secondary pneumothorax with tension physiology
Discussion
The patient’s clinical presentation of chest pain, dyspnea, dry cough, and physical exam demonstrating absence of breath sounds, along with confirmatory imaging, is all most consistent with spontaneous pneumothorax. Other common physical exam signs seen in pneumothorax include decreased breath sounds, tactile fremitus and hyper-resonance to percussion. Her chest x-ray showed loss of right-sided lung markings with a deep sulcus sign (black arrow, Figure 1B), which is a deep costophrenic angle ipsilateral to the side of the pneumothorax. Secondary pneumothorax, rather than primary, is more consistent with the patient’s family history of pneumothorax and skin findings of fibrofolliculomas, which are a type of skin hamartoma (Figure 3). Our patient has Birt-Hogg-Dubé syndrome (BHDS), which is a hereditary syndrome with pulmonary cysts, secondary spontaneous pneumothorax, and skin hamartomas. BHDS is a classic, but rare, cause of secondary pneumothorax1.
A computed tomography (CT) of the chest was performed prior to her presentation to the emergency department, which showed bilateral cystic lung lesions (Figure 2A). On presentation to the emergency department, the initial chest x-ray showed a large right sided tension pneumothorax (2B, arrows). She underwent emergent chest tube placement with improvement of her symptoms. She proceeded to right sided video-assisted thoracoscopic surgery (VATS) with partial pleurectomy and mechanical pleurodesis (Figure 2C) given her risk of recurrence of secondary spontaneous pneumothorax in the setting of BHDS. Following the procedure, she had resolution of the right-sided pneumothorax, but developed new subcutaneous air (arrow), which was managed conservatively. Chest x-ray 1 month later showed complete resolution of the pneumothorax, mediastinal emphysema, and subcutaneous emphysema (2D). Long-term follow-up did not demonstrate recurrence of secondary spontaneous pneumothorax.
Figure 2: (A-D)
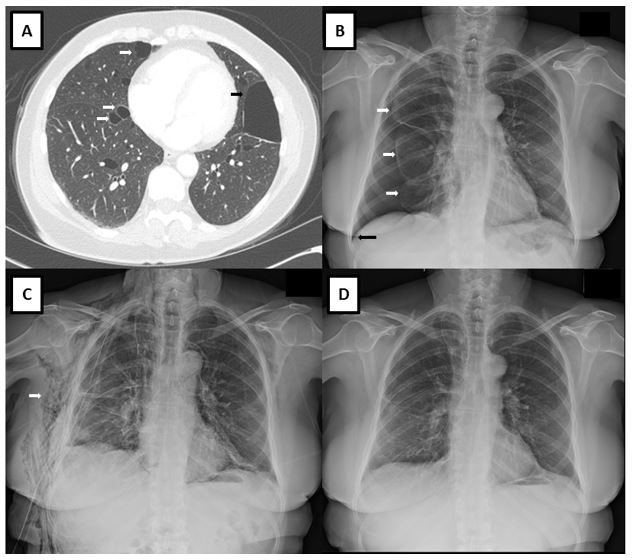
Figure 3: Fibrofolliculoma

Pneumothorax is a clinical diagnosis, and imaging is used to confirm the diagnosis. The patient’s clinical presentation makes malignant pleural effusion, COPD exacerbation, and community acquired pneumonia less likely. An upright posteroanterior chest radiograph can help confirm the diagnosis if absence of lung markings, deep sulcus sign, and mediastinal shift are demonstrated3. Given the contralateral mediastinal shift on our patient’ chest radiograph (Figure 2B), there is evidence of tension physiology without hemodynamic compromise. However, tension physiology on chest x-ray can portend hemodynamic decline, and therefore, clinicians should have high clinical suspicion for pneumothorax as waiting on results of chest x-ray may result in clinical decompensation. Spontaneous pneumothorax is classified as primary or secondary depending on the presence or absence of underlying lung disease. Primary pneumothorax occurs without underlying lung disease or precipitating event, whereas secondary pneumothorax can occur in a variety of lung pathology1,3. The differential diagnosis for secondary spontaneous pneumothorax includes underlying lung disease (COPD with emphysema, cystic fibrosis, severe asthma, BHDS), infections (bacterial pneumonia, Pneumocystis jirovecii pneumonia, tuberculosis), interstitial lung disease (sarcoidosis, idiopathic pulmonary fibrosis, lymphangioleiomyomatosis, histiocytosis X), connective tissue and autoimmune disease, and lung malignancy3. Secondary causes of pneumothorax tend to be more severe and life-threatening given the underlying lung disease, and require more prompt evaluation and treatment3.
BHDS is an autosomal dominant syndrome with 600 families described world-wide, although it is likely underdiagnosed1. The mutation is in a tumor suppressive gene encoding for the folliculin protein, and our patient had a known folliculin (FLN-C) gene mutation1,4. The syndrome involves the lungs, skin, and kidneys, with lung cysts as the hallmark feature present in 67-90% of patients1. Cysts tend to appear in lower lung bases with thin-walls and irregular, variable shapes1. Patients have skin hamartomas, and most commonly fibrofolliculomas, which are white dome shaped papules usually located on face and neck5. Patients also have increased risk of renal tumors, and should undergo routine surveillance1. Penetrance of clinical manifestations of disease varies within families6. BHDS may first present with a spontaneous pneumothorax unless a family history of disease is known5. There is a 50-fold increased risk of pneumothorax with 40-75% of patients experiencing at least one spontaneous pneumothorax1. Due to this risk, early pleurodesis is recommended6. Clinicians should routinely consider secondary causes for patients presenting with pneumothorax, as this changes management of pneumothorax treatment. Awareness of inherited causes of secondary pneumothorax in patients is critical to appropriate diagnosis and management of patients with secondary pneumothorax.
References:
-
Jensen DK, Villumsen A, Skytte AB, Madsen, MG, Sommerlund M, Bendstrup E. Birt–Hogg–Dubé syndrome: a case report and a review of the literature. European Clinic Respiratory Journal. 2017; 4: 1, 1292378.
-
Fibrofolliculoma. NCI. Christine Ko. Published April 22, 2015. https://visualsonline.cancer.gov/details.cfm?imageid=10027. .
-
Noppen M, De Keukeleire T. Pneumothorax. Respiration. 2008;76(2):121-7.
-
Skolnik K, Willis TH, Dornan K, Perrier R, Burrowes PW, Davidson WJ. Birt-Hogg-Dubé syndrome: a large single family cohort. Respiratory Research. 2016; 17:22.
-
Bock K, Lohse Z, Madsen PH, Hilberg O. Birt-Hogg-Dubé syndrome: spontaneous pneumothorax as a first symptom. BMJ Case Rep. 2018 Jan 9;2018. pii: bcr-2017-219979. doi: 10.1136/bcr-2017-219979.
-
Gupta N, Seyama K, McCormack FX, et al. Pulmonary manifestations of Birt-Hogg-Dubé syndrome. Fam Cancer 2013; 12:387–96.


