A stranger in the lung
Nitin Sabharwal1 M.B.B.S, Sushilkumar Satish Gupta2 M.D., Shyam Shankar2 M.B.B.S., Chanaka Seneviratne3 M.D.
1Department of Internal Medicine, Maimonides Medical Center, Brooklyn, NY, USA.
2 Department of Pulmonary and Critical Care Medicine, Maimonides Medical Center, Brooklyn, NY, USA.
3Attending, Department of Pulmonary and Critical Care Medicine, Maimonides Medical Center, Brooklyn, NY, USA.
* The authors report no financial relationships or conflicts of interest regarding the content herein.
* There was no financial support related to the content herein.
Case
A 64-year-old male with a past medical history of hypertension and diabetes presented at our emergency room (ER) with complaints of fever, non-productive cough with pleuritic chest pain for one week. He failed outpatient oral antibiotic therapy and was sent to the hospital for further management. In the ER, he was febrile up to 102oF and had leukocytosis of 15.6 X 109/L with neutrophilia of 90.3%. A bedside ultrasound was performed which is shown in video 1.
Video 1: Ultrasound video on a phased array probe shows the swirling movement of the cellular debris, fibrin strands and septations in the pleural cavity.
Question
What is the most appropriate test that should be requested for this patient?
- Thoracentesis followed by antibiotics
- Non-invasive positive pressure ventilation for atelectasis.
- Diuresis with intravenous furosemide.
- Needle decompression of tension pneumothorax
A: ) Thoracentesis followed by antibiotics
Discussion
The patient was found to have pneumonia in the right lower lobe, which resulted in a parapneumonic effusion. Parapneumonic effusions occur due to increased passage of interstitial fluid as a result of pneumonia and are exudative in nature. Parapneumonic effusions can be further classified as uncomplicated, complicated and empyema. Complicated pleural effusions appear as exudative effusions on lung ultrasounds and have a non-homogenous echogenic pattern due to cellular debris, fibrin strands and septations. Cardiac and respiratory movements lead to swirling movements of these cellular debris, fibrin strands and septations, giving us a dynamic presentation of pleural effusion on ultrasound imaging. The presence of cellular debris and septations in parapneumonic effusions may indicate the presence of empyema or a complicated parapneumonic effusion which requires drainage and a longer duration of antibiotics.(1)
The patient demonstrated clinical signs of infection with an exudative unilateral effusion and therefore would not require any of the above-mentioned management strategies except for thoracentesis and antibiotics. Noninvasive positive pressure ventilation was deemed non-beneficial as the atelectasis of the lung was as a result of pleural effusion. Diuretics for pleural effusions are helpful only when the effusion is due to heart failure or pathologies which lead to increased hydrostatic pressure within the pulmonary vasculature, which were not the causes in our case. Such effusions are generally bilateral and transudative in nature. The patient did not have a pneumothorax so did not require needle decompression.
Bedside lung ultrasounds (LUS), when performed by experienced physicians, are more sensitive than a chest radiograph (CXR) in the diagnosis of a pleural effusion, having a sensitivity of 100% compared to CXR which is only 65%.(2) LUS has the ability of detecting pleural effusions as small as 3-5 ml with an added advantage of defining the complexity of the effusion better than a chest computed tomography (CT) (3).
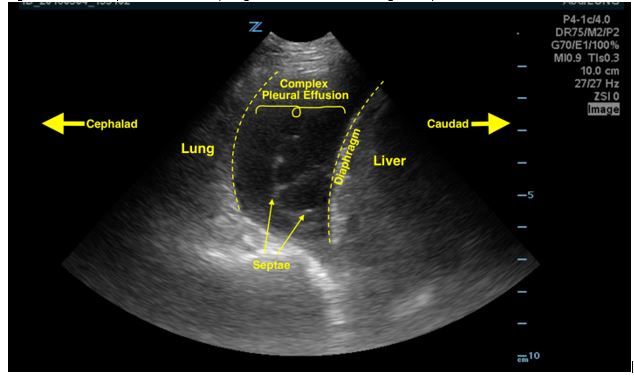
In order to identify a pleural effusion, intensivists must first locate important anatomical landmarks which include the chest wall, diaphragm and sub-diaphragmatic structures, such as the spleen or the liver and the lung (Figure 1). Once identified, the effusion can be further described by its echogenicity and quantification.
Transudative effusions are generally anechoic. However, a very cellular transudative effusion can be homogenously echoic (4). Exudative effusion, on the other hand, can be homogenously echoic or non-homogenous echoic due to cellular debris, fibrin strands and septations like in the case described.
LUS can help aid management of the pleural effusion primarily by allowing quantification and echogenic classification of the pleural effusion. Pleural effusions may be quantified into small, moderate and large effusion categories. However, for an accurate estimation, the following formula can be used: volume of pleural fluid in milliliters = 20 × (distance between visceral and parietal pleura in millimeters).(5) Thoracentesis remains the mainstay in management of parapneumonic pleural effusions, empyema and hemothorax.
References
-
Koppurapu V, Meena N. A review of the management of complex para-pneumonic effusion in adults. J Thorac Dis. 2017;9(7):2135-41.
-
Xirouchaki N, Magkanas E, Vaporidi K, Kondili E, Plataki M, Patrianakos A, et al. Lung ultrasound in critically ill patients: comparison with bedside chest radiography. Intensive Care Med. 2011;37(9):1488-93.
-
Lichtenstein D, Goldstein I, Mourgeon E, Cluzel P, Grenier P, Rouby JJ. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology. 2004;100(1):9-15.
-
Yang PC, Luh KT, Chang DB, Wu HD, Yu CJ, Kuo SH. Value of sonography in determining the nature of pleural effusion: analysis of 320 cases. AJR Am J Roentgenol. 1992;159(1):29-33.
-
Balik M, Plasil P, Waldauf P, Pazout J, Fric M, Otahal M, et al. Ultrasound estimation of volume of pleural fluid in mechanically ventilated patients. Intensive Care Med. 2006;32(2):318.
Figure 1: Anechoic space above the diaphragm with visible linear echogenic septations.