A Plateau of Flow
Daniel J da Costa MD, David W Hsia MD
Division of Respiratory and Critical Care Physiology and Medicine
Harbor-UCLA Medical Center
Case
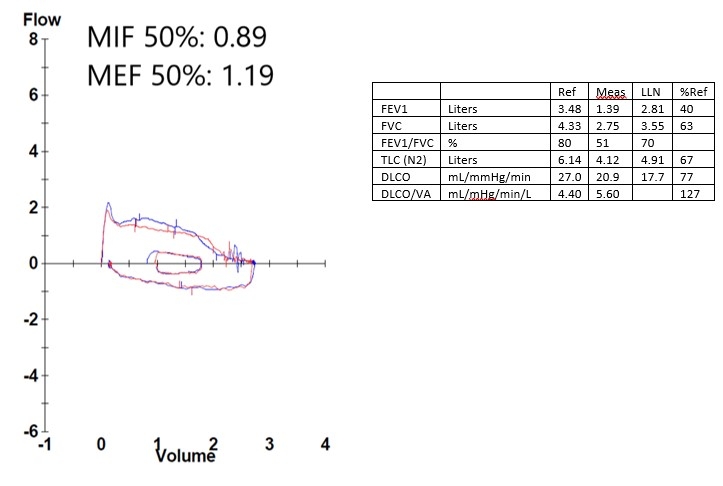
A 41-year-old male with a history of prior tracheostomy due to a motor vehicle accident presented to our emergency department with dyspnea. Physical examination revealed stridor with otherwise normal range vital signs. Pulmonary function tests were obtained as seen here.
Question
What is the diagnosis?
- Fixed upper airway obstruction
- Variable intrathoracic upper airway obstruction
- Left mainstem bronchus obstruction
- Variable extrathoracic airway obstruction
D: Variable extrathoracic airway obstruction
Discussion
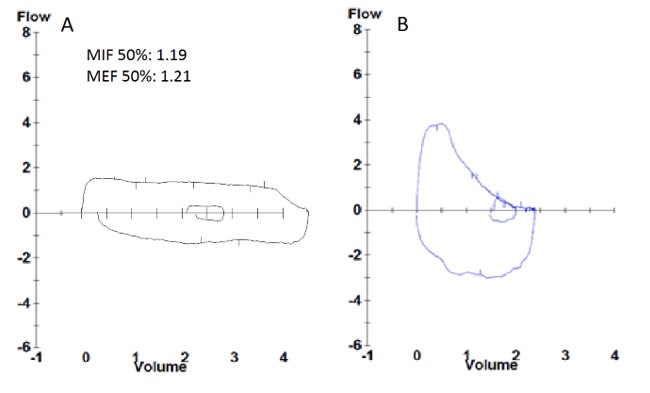
This patient has a flow-volume loop demonstrating a flattening of both the inspiratory and expiratory limbs raising concern for an upper airway obstruction. When determining if the obstruction is intrathoracic or extrathoracic, we need to assess if the flow limitation is equal or different between inspiration and expiration. To do this, we can look at the ratio of maximal inspiratory flow at 50% FVC (MIF50%) to maximal expiratory flow at 50% FVC (MEF50%) (1,2). A ratio near 1 would indicate a fixed obstruction; a higher ratio can indicate intrathoracic lesions while lower ratios can indicate extrathoracic lesions, as in this patient. In regards to the incorrect answers, answer A (fixed airway obstruction) would have the inspiratory and expiratory limbs limited at the same flow rate as seen in the figure below, panel A. Answer B (Variable intrathoracic upper airway obstruction) would have the expiratory flow limb more limited than the inspiratory flow which is the opposite of which was seen in our patient. Answer C is incorrect as you would expect a biphasic flow volume loop in both expiratory and inspiratory limbs.
The physiologic reason for a variable obstruction is attributed to compression due to changes in transmural pressure (2). During inspiration, intraluminal pressure become more negative relative to atmospheric pressure leading to worsening obstruction of flow in the setting of extrathoracic lesions. An opposite effect happens for intrathoracic lesions. During expiration, pleural pressure will become positive when compared to intratracheal pressure, which can lead to worsening obstruction of flow in the setting of an intrathoracic upper airway lesion. This patient had a variable extrathoracic upper airway obstruction due to tracheal stenosis as a late complication of his prior tracheostomy. In addition to spirometry, this patient had a CT scan which confirmed stenosis. He subsequently underwent bronchoscopic intervention and dilation. Post procedure, his flow volume loop normalized as below, panel B.
References
-
Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Series "ATS/ERS Task Force: Standardisation of lung function testing". Eur Respir J 2005; 26: 948-68.
-
Gamsu G, Borson DB, Webb WR, et al. Structure and function in tracheal stenosis. Am Rev Respir Dis. 1980; 121(3): 519–31.


