A Black Rose in the Airway
Mohamad Badr Jandali, MD, Seth Sklare, MD, Andreas Schmid, MD
Kansas University Medical Center, Department of Pulmonary and critical care Medicine
Case
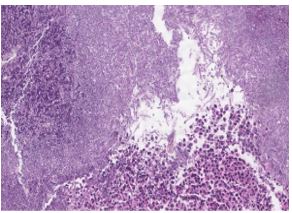
A 73-year-old female presents with progressive cough and dyspnea on exertion. She denies hemoptysis, weight loss or night sweats. She reports no recent travel history or tuberculosis exposure. She is a former smoker (60 packs-years) with a history of remote non-small cell lung cancer in the right upper lobe, treated with chemoradiation and resection 14 years ago. She also has rheumatoid arthritis and is being treated with hydroxychloroquine and methotrexate. Her rheumatism has had no extraarticular manifestations and has been under good control. Patient had an abnormal chest film showing left upper lobe consolidation. Representative sections of a chest CT scan are shown below (Images 1 & 2). Diagnostic bronchoscopy was performed which revealed the findings in Image 3. Rest of the bronchoscopic examination was unremarkable.
Image 1
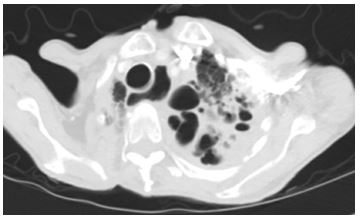
Image 2
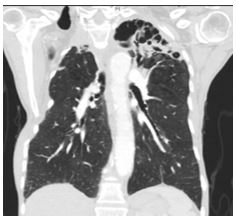
Image 3

Question
What is the abnormality observed during bronchoscopy?
- Tuberculosis
- Aspergillosis
- Recurrent Non-Small Cell Lung Cancer
- Amyloidosis
Answers: B. Aspergillosis
Discussion
This case is a rare presentation of endobronchial aspergillosis, characterized by the growth of aspergillus into the bronchial lumen. Aspergillosis is a spectrum of diseases. The most common categories are aspergilloma (image 4), invasive aspergillosis (image 5) and allergic bronchopulmonary aspergillosis (ABPA) (image 6). Less common presentations are subacute invasive aspergillosis and aspergillus tracheobronchitis. There are few reports of endobronchial aspergillosis in the literature. It can present as an isolated finding or with other forms of pulmonary aspergillosis. Most common symptoms are hemoptysis, dyspnea and cough. Diagnosis usually requires histopathological examination, as a small case series suggested the diagnostic yield of bronchial lavage was only 16.7%.
Our patient was diagnosed with endobronchial aspergillosis after the endobronchial biopsy of the right main bronchus lesion showed abundance of septate acute angle branching hyphae suggestive of aspergillus (image 7). This was confirmed by the growth of Aspergillus niger on same tissue culture. Her left upper lobe bronchoalveolar lavage also grew Aspergillus niger. Given the left upper lobe involvement, she was diagnosed with subacute invasive aspergillosis as well, for which she was started on a long course of itraconazole. However, treatment of isolated endobronchial aspergillosis is not clear. There are reports of incidental cases that were observed without complications but antifungals and even surgery have been used in the past.
Image 4
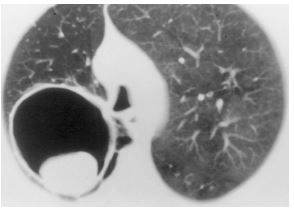
Image 5
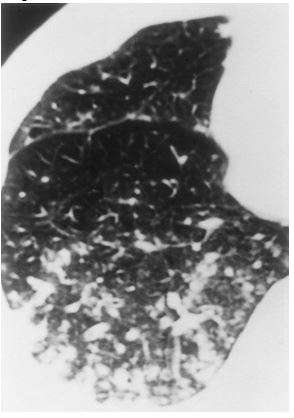
Image 6
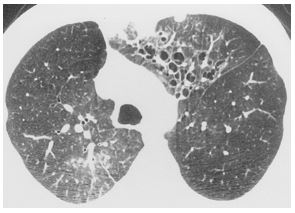
Image 7
References:
-
Kim JS, Rhee Y, Kang SM, et al. A case of endobronchial aspergilloma. Yonsei Med J 2000; 41: 422–5.
-
Qureshi MA, Nair VS. Pulmonary aspergilloma: Bronchoscopic appearance. J Bronchol 2003; 10: 204–6.
-
Huang, D., Li, B., Chu, H., et. al. Endobronchial aspergilloma: A case report and literature review. Experimental and Therapeutic Medicine 2017; 14.1: 547-54.
-
Ma JE, Yun EY, Kim YE, et. al. Endobronchial aspergilloma: report of 10 cases and literature review. Yonsei Med J 2011; 52(5): 787-92.
-
Franquet T, Müller N, Giménez A et al. Spectrum of pulmonary aspergillosis: histologic, clinical, and radiologic findings. Radiographics 2001; 21: 825–37.


