Reviewed By Clinical Problems Assembly
Submitted by
Leanne K. Strack, DO
Clinical Instructor and Pulmonary/Critical Care Fellow
The Ohio State University
Columbus, Ohio
James M. O'Brien, MD
Associate Professor of Medicine, Pulmonary/Critical Care Medicine
The Ohio State University
Columbus, Ohio
Submit your comments to the author(s).
History
An 18-year-old man presents to the emergency department stating he felt like he “was going to die.” While on break at work, he experienced sudden onset sharp, midsternal chest pain. He had no dyspnea or radiation of the pain. He had not suffered any recent chest trauma but did strike his head on a piece of equipment at work without sequelae. Three days prior to presentation he had cough productive of yellow sputum without fevers or chills. At the time of evaluation, the pain had been present for several hours and was only relieved by narcotic medications.
His past medical history was significant for bipolar disorder, which was controlled without medications. He worked as a stock clerk at a department store. He was a current smoker, 1 pack per day for 2 years, and he gave a history of prior cocaine use, but denied any recent illicit drug usage.
Physical Exam
Lab
Figures

Figure 1. Erect Posteroanterior (AP) Chest Radiograph.
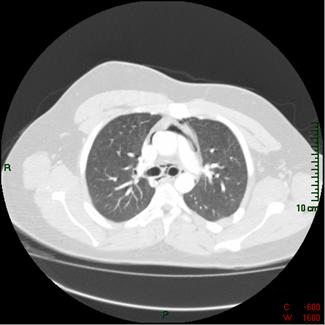
Figure 2. Computed Tomography (CT) Scan of the Chest.
References
- Macia I, Moya J, Ramos R, Moerea R, Escobar I, Saumench J, Perna V, Rivas F. Spontaneous pneumomediastinum: 41 cases. Eur J Cardiothorac Surg 2007;31:1110-1114.
- Newcomb AE, Clarke CP. Spontaneous pneumomediastinum a benign curiosity or a significant problem. Chest 2005;128:3298-3308.
- Fugo JR, Reade CC, Kypson AP. Spontaneous pneumomediastinum. Curr Surg 2006;63:351-353.
- Mondello B, Pavia R, Ruggeri P, Barone M, Barresi P, Monaco M. Spontaneous pneumomediastinum: experience in 18 adult patients. Lung 2007;185:9-14.
- Freixinet J, Garcia F, Rodriguez PM, Santana NB, Quintero CO, Hussein M. Spontaneous pneumomediastinum long-term follow-up. Respir Med 2005;99:1160-1163.
- Langweiler TE, Steffani KD, Bogoevski DP, Mann O, Izbicki JR. Spontaneous pneumomediastinum. Ann Thorac Surg 2004; 78:711-713.


