"Horse play and the Lung" - a possible cobalt effect?
Reviewed By Environmental & Occupational Health Assembly
Submitted by
Husam M. Abdel-Qadir
Postgraduate trainee in Internal Medicine
Toronto Western Hospital
Toronto, Canada
Marcos M Ribeiro MD
Clinical Research Fellow
Toronto Western Hospital
Toronto, Canada
William Geerts MD
Professor
Department of Medicine
University of Toronto
Toronto, Canada
Adam Wisnewski PhD
Associate Professor
Department of Internal Medicine
Yale University School of Medicine
Connecticut, USA
Susan M Tarlo M.B, B.S
Professor
Department of Medicine
University of Toronto
Toronto, Canada
Submit your comments to the author(s).
History
A 38-year-old female horse-farmer was referred to us with a history of respiratory symptoms beginning on the day she started to use a new, finely powdered, horse-feed supplement. She developed dyspnea immediately after exposure and later that day noted a nonproductive cough, lightheadedness, and chest discomfort. Over the following week, the cough continued and she noted mild wheezing, progressive exertional dyspnea, and upper chest tightness exacerbated by activity such as climbing one flight of stairs. These symptoms prompted her to make an emergency department visit. She had no fever, chills, arthralgias, or hemoptysis. She was an ex-smoker for 18 months after a 7 pack-year history. Past medical history and review of systems were remarkable only for a history of childhood asthma, which was triggered by unusually high exposures to dust and horses. This required only rare short-acting bronchodilator use and had improved by the age of 12. She also had symptoms to suggest mild allergic rhinitis in the spring.
Physical Exam
Physical examination one week after the onset of her symptoms revealed no respiratory distress at rest. She was afebrile with normal vital signs, respiratory rate was 20/minute, and oxygen saturation at rest was 98% on room air. There was no clubbing or lymphadenopathy and chest examination was normal. There were no crackles or wheezes. The jugular venous pressure was not increased and cardiovascular examination was normal. A complete blood count (CBC) and differential white blood cell count (WBC) were unremarkable. A chest radiograph showed diffuse hazy opacities in the lungs bilaterally (Figure 1 and 2). She was referred for pulmonary outpatient assessment.
Figures
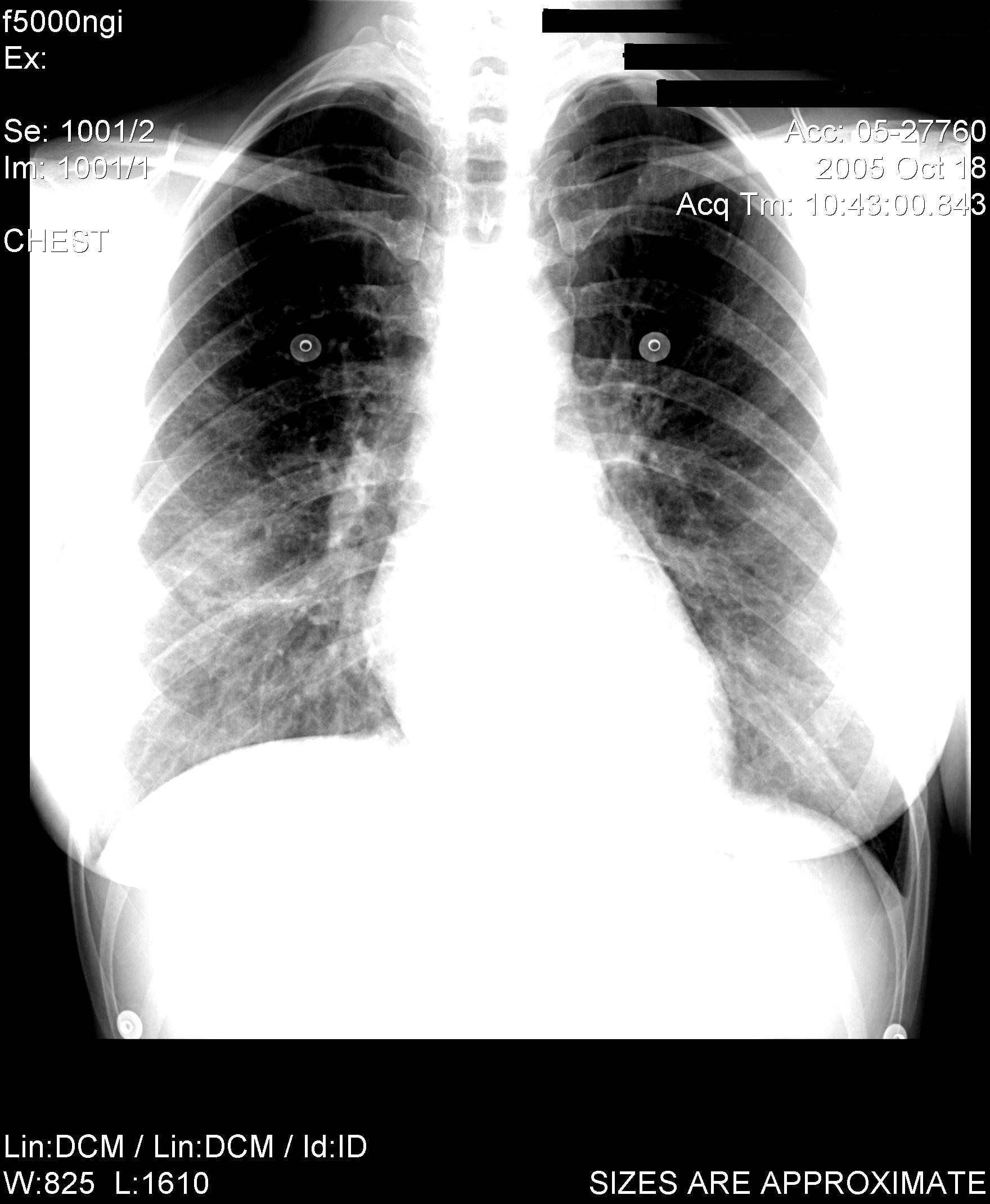
Figure 1: Chest radiograph 1 week after symptom onset
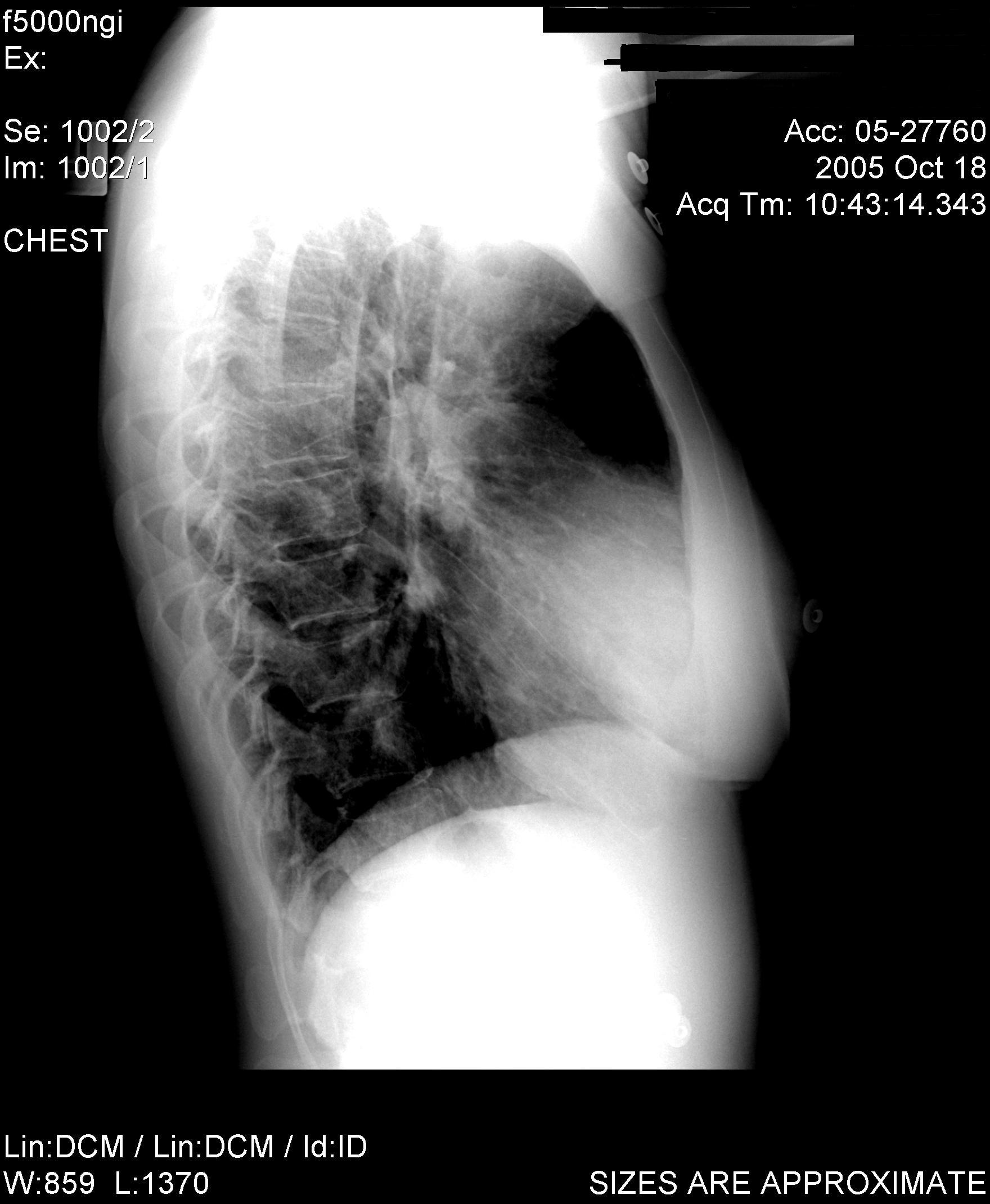
Figure 2: Chest radiograph 1 week after symptom onset
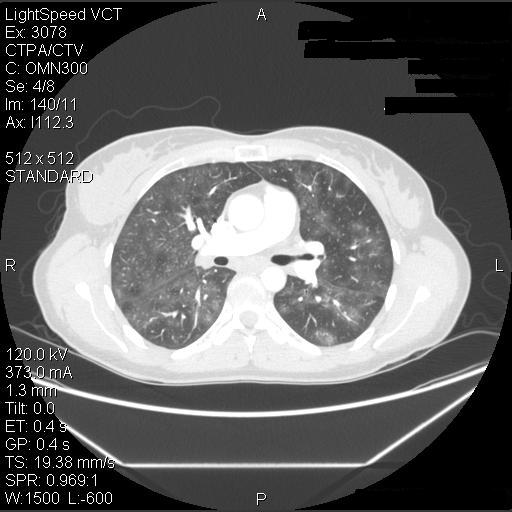
Figure 3: Chest CT 1 month after the onset of symptoms

Figure 4: Transbronchial biopsy
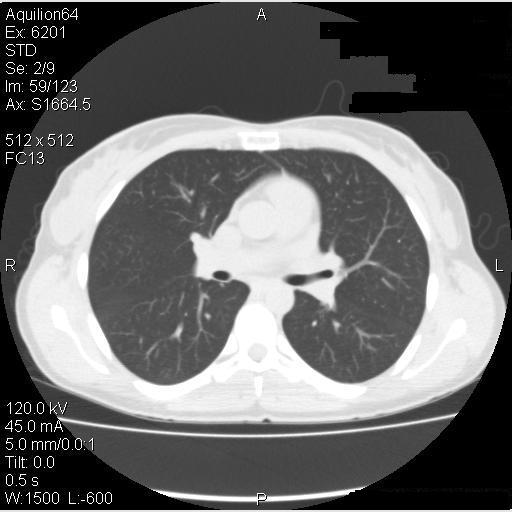
Figure 5: High resolution CT scan at 6 months
References
- Mohr LC. Hypersensitivity pneumonitis. Curr Opin Pulm Med 2004;10:401-411
- Ismail T, McSharry C, Boyd G. Extrinsic allergic alveolitis. Respirology 2006;11:262-268.
- Krakowiak A, Dudek W, Tarkowski M, Swiderska-Kielbik S, Niescierenko E, Palczynski C. Occupational asthma caused by cobalt chloride in a diamond polisher after cessation of occupational exposure: a case report. Int J Occup Med Environ Health 2005;18:151-158.
- Linna A, Oksa P, Palmroos P, Roto P, Laippala P, Uitti J. Respiratory health of cobalt production workers. Am J Ind Med 2003;44:124-132.
- Kusaka Y, Iki M, Kumagai S, Goto S. Epidemiological study of hard metal asthma. Occup Environ Med 1996;53:188-193.
- Sjogren I, Hillerdal G, Andersson A, Zetterstrom O. Hard metal lung disease: importance of cobalt in coolants. Thorax 1980;35:653-659.
- May JJ, Stallones L, Darrow D, Pratt DS. Organic dust toxicity (pulmonary mycotoxicosis) associated with silo unloading. Thorax 1986;41:919-923.
- Nemery B, Verbeken EK, Demedts M. Giant cell interstitial pneumonia (hard metal lung disease, cobalt lung). Semin Respir Crit Care Med 2001;22:435-448
- Cugell DW. The hard metal diseases. Clin Chest Med 1992;13:269-279.
- Migliori M, Mosconi G, Michetti G, Belotti L, D'Adda F, Leghissa P, Musitelli O, Cassina G, Motta T, Seghizzi P, Sabbioni E. Hard metal disease: eight workers with interstitial lung fibrosis due to cobalt exposure. Sci Total Environ 1994;150:187-196
- Lison D, Lauwerys R, Demedts M, Nemery B. Experimental research into the pathogenesis of cobalt/hard metal lung disease. Eur Respir J 1996;9:1024-1028.
- Kreiss K. Beryllium and cobalt. In: Textbook of Occupational and Environmental Medicine, Rosenstock L, Cullen MR, Brodkin CA, Redlich CA, editors. 2nd ed. Philadelphia, PA: Elsevier, Saunders; 2005. p. 950-954.
- Nemery B, Abraham JL. Hard metal lung disease: still hard to understand. Am J Respir Crit Care Med 2007;176:2-3


