Reviewed By Sleep and Respiratory Neurobiology Assembly
Submitted by
Dries Testelmans, MD, PhD
Fellow
Department of Pulmonology
University Hospitals Leuven
Leuven, Belgium
Natalia Siyanko, MD
Fellow
Sleep Laboratory and EFCR, Department of Rehabilitation and Physiology
UniversityHospital Grenoble
Grenoble, France
Renaud Tamisier MD, PhD
Associate Professor of Physiology
Sleep Laboratory and EFCR, Department of Rehabilitation and Physiology
UniversityHospital Grenoble
Grenoble, France
Submit your comments to the author(s).
History
A 56-year old man with a history of ischemic chronic heart failure was referred to our clinic in order to be screened for associated pulmonary conditions. Four weeks prior, he had undergone a double coronary artery bypass following an acute myocardial ischemia episode. The patient had no history of cerebrovascular or metabolic disease and stopped smoking since his surgery. Two weeks after surgery, he started a cardiac rehabilitation program. According to the cardiologist, the patient was clinically stable, asymptomatic and no new medication was planned to be introduced. The left ventricular ejection fraction (LVEF) was 34%.
The patient had NYHA class II dyspnea, but did not complain about dyspnea during sleep. He did not report snoring, or daytime sleepiness; he had an Epworth Sleepiness Score of 6.
Physical Exam
Physical Examination
The patient had a height of 173 cm and weighed 49 kg; his BMI was 16.4 kg/m2. Respiratory and cardiovascular examinations were normal and no signs of pulmonary edema were found. His blood pressure was 130/70 mmHg, with a heart rate of 62 beats/min.
Pulmonary function test
FEV1: 2.68 L (80% predicted) - FVC: 4.04 L (97% predicted) - FEV1/FVC 0.66 -TLC: 7.96 L (118% predicted)
Arterial blood gases: PaO2: 97.2 mmHg - PaCO2: 32.3 mmHg - pH: 7.39 – HCO3-: 19.2 mmol.l-1 – SaO2: 98%
Figure 1 and 2:
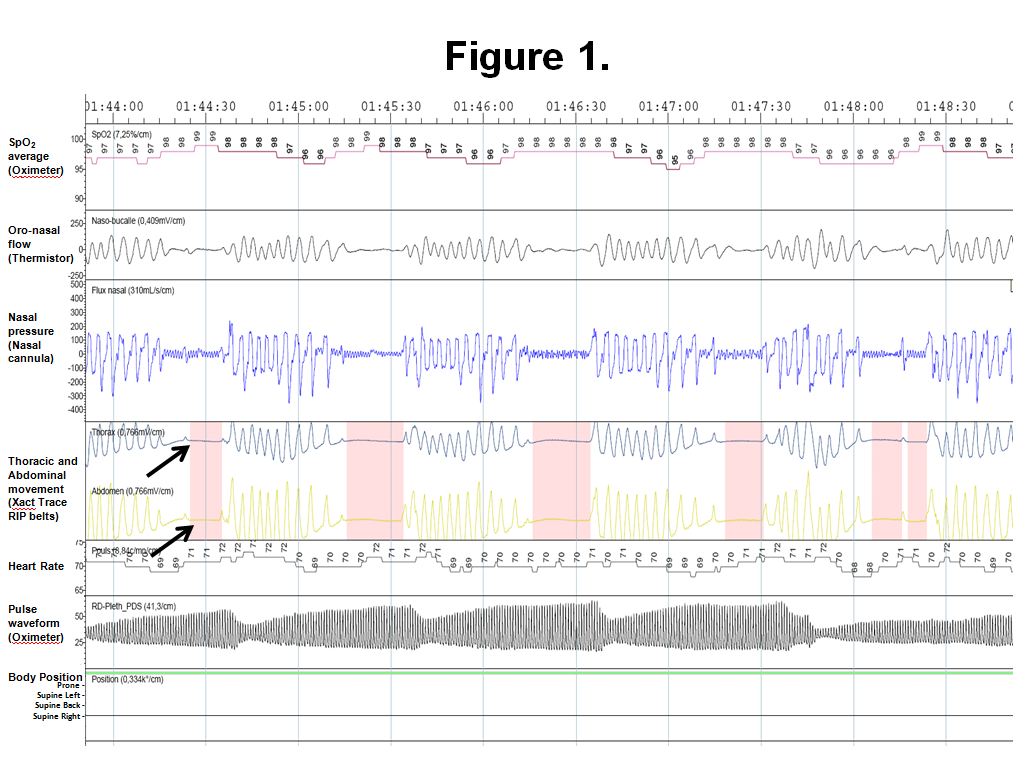
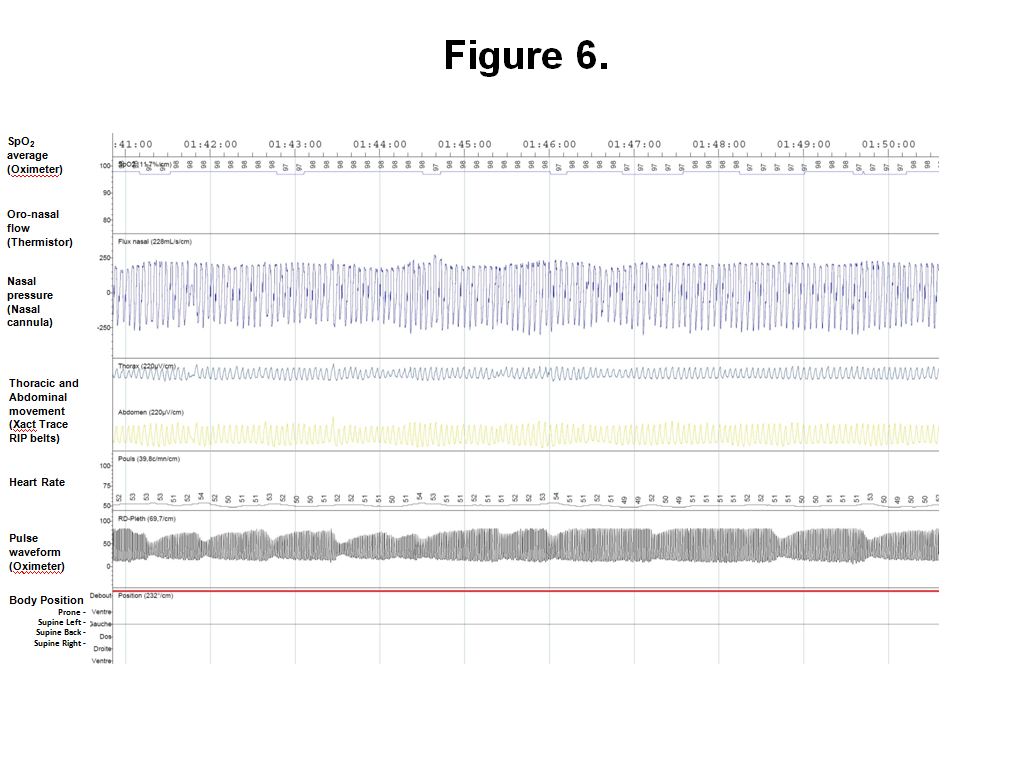
Figure 1: Representative trace of recorded sleep study showing typical central respiratory events followed by hyperventilation. Note the absence of respiratory effort on thoracic and abdominal belts (see arrows). Most of apneic events are responsible for significant desaturations, with changes in heart rate despite the patient being on beta-blockers and severe peripheral vasoconstriction as assessed by the decrease in finger pulse wave oximetry amplitude.
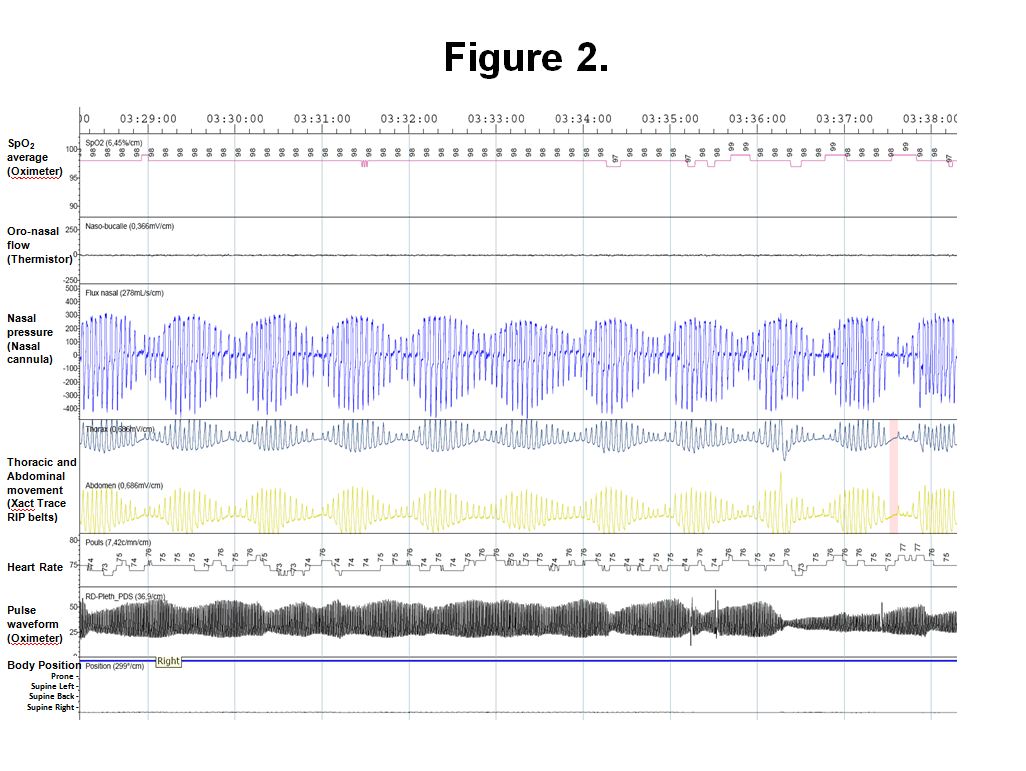
Figure 2: Representative trace of a 10-minute recorded ventilation during the sleep study showing typical Cheyne-Stokes Respiration (CSR). CSR is defined by 3 consecutive cycles of cyclical crescendo and decrescendo change in breathing amplitude (Figure 2) and at least 1 of the following: 1) Five or more central apneas or hypopneas per hour of sleep and/or 2) The cyclic crescendo and decrescendo change in breathing amplitude has a duration of at least 10 consecutive minutes.
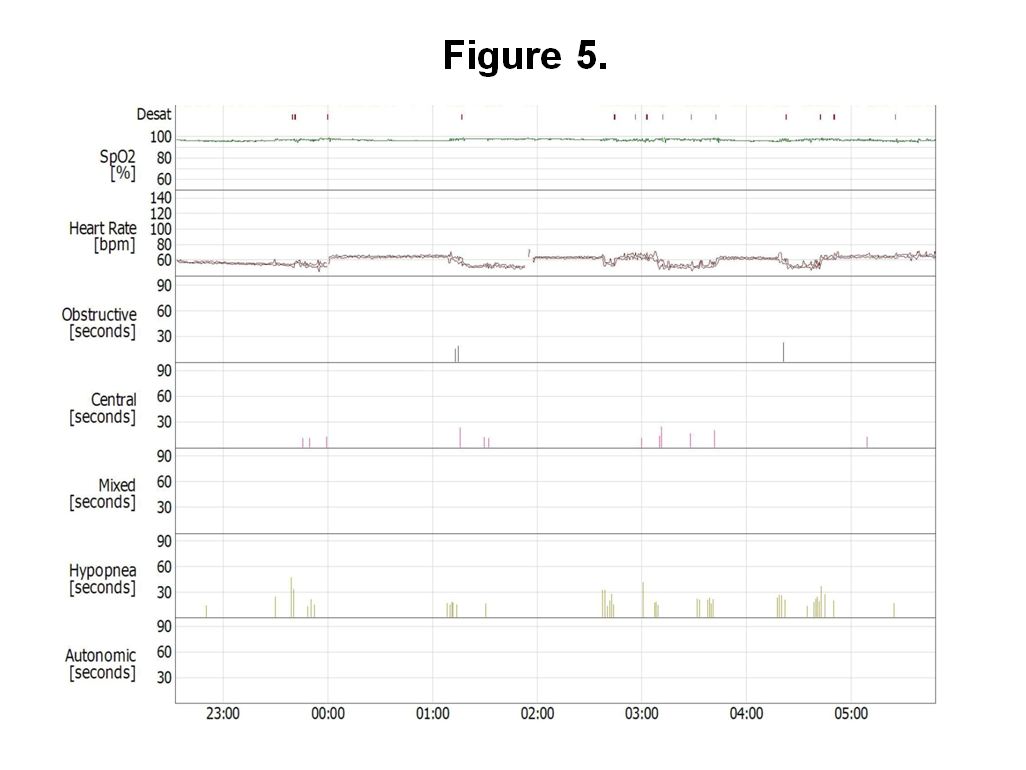
Diagnostic Respiratory Polygraphy: The total apnea/hypopnea index (AHI) was 34.5 per hour with an obstructive AI of 0.1 and a central AI of 19.9 per hour. During the night, there was no pronounced drop in oxygen saturation (SpO2), with the lowest SpO2 of 95% and a mean SpO2 of 98%.
References
- Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. The report of an american academy of sleep medicine task force. Sleep 1999;22:667-689.
- Oldenburg O, Lamp B, Faber L, Teschler H, Horstkotte D, Topfer V. Sleep-disordered breathing in patients with symptomatic heart failure: A contemporary study of prevalence in and characteristics of 700 patients. Eur J Heart Fail 2007;9:251-257.
- Tremel F, Pepin JL, Veale D, Wuyam B, Siche JP, Mallion JM, Levy P. High prevalence and persistence of sleep apnoea in patients referred for acute left ventricular failure and medically treated over 2 months. Eur Heart J 1999;20:1201-1209.
- Lanfranchi PA, Braghiroli A, Bosimini E, Mazzuero G, Colombo R, Donner CF, Giannuzzi P. Prognostic value of nocturnal cheyne-stokes respiration in chronic heart failure. Circulation 1999;99:1435-1440.
- Sin DD, Fitzgerald F, Parker JD, Newton G, Floras JS, Bradley TD. Risk factors for central and obstructive sleep apnea in 450 men and women with congestive heart failure. Am J Respir Crit Care Med 1999;160:1101-1106.
- Javaheri S, Corbett WS. Association of low paco2 with central sleep apnea and ventricular arrhythmias in ambulatory patients with stable heart failure. Ann Intern Med 1998;128:204-207.
- Solin P, Bergin P, Richardson M, Kaye DM, Walters EH, Naughton MT. Influence of pulmonary capillary wedge pressure on central apnea in heart failure. Circulation 1999;99:1574-1579.
- Dempsey JA. Crossing the apnoeic threshold: Causes and consequences 10.1113/expphysiol.2004.028985. Exp Physiol 2005;90:13-24.
- Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F, Falk V, Filippatos G, Fox K, Huber K, Kastrati A, Rosengren A, Steg PG, Tubaro M, Verheugt F, Weidinger F, Weis M. Management of acute myocardial infarction in patients presenting with persistent st-segment elevation: The task force on the management of st-segment elevation acute myocardial infarction of the european society of cardiology. Eur Heart J 2008;29:2909-2945.
- Oldenburg O, Bitter T, Wiemer M, Langer C, Horstkotte D, Piper C. Pulmonary capillary wedge pressure and pulmonary arterial pressure in heart failure patients with sleep-disordered breathing. Sleep Med 2009;10:726-730.
- Garrigue S, Bordier P, Jais P, Shah DC, Hocini M, Raherison C, Tunon De Lara M, Haissaguerre M, Clementy J. Benefit of atrial pacing in sleep apnea syndrome. N Engl J Med 2002;346:404-412.
- Sinha AM, Skobel EC, Breithardt OA, Norra C, Markus KU, Breuer C, Hanrath P, Stellbrink C. Cardiac resynchronization therapy improves central sleep apnea and cheyne-stokes respiration in patients with chronic heart failure. J Am Coll Cardiol 2004;44:68-71.
- Szollosi I, O'Driscoll DM, Dayer MJ, Coats AJ, Morrell MJ, Simonds AK. Adaptive servo-ventilation and deadspace: Effects on central sleep apnoea. J Sleep Res 2006;15:199-205.
- Teschler H, Dohring J, Wang YM, Berthon-Jones M. Adaptive pressure support servo-ventilation: A novel treatment for cheyne-stokes respiration in heart failure. Am J Respir Crit Care Med 2001;164:614-619.
- Javaheri S, Parker TJ, Wexler L, Liming JD, Lindower P, Roselle GA. Effect of theophylline on sleep-disordered breathing in heart failure. N Engl J Med 1996;335:562-567.
- Javaheri S. Acetazolamide improves central sleep apnea in heart failure: A double-blind, prospective study. Am J Respir Crit Care Med 2006;173:234-237.
- Philippe C, Stoica-Herman M, Drouot X, Raffestin B, Escourrou P, Hittinger L, Michel PL, Rouault S, d'Ortho MP. Compliance with and effectiveness of adaptive servoventilation versus continuous positive airway pressure in the treatment of cheyne-stokes respiration in heart failure over a six month period. Heart 2006;92:337-342.
- Sin DD, Logan AG, Fitzgerald FS, Liu PP, Bradley TD. Effects of continuous positive airway pressure on cardiovascular outcomes in heart failure patients with and without cheyne-stokes respiration. Circulation 2000;102:61-66.
- Arzt M, Harth M, Luchner A, Muders F, Holmer SR, Blumberg FC, Riegger GA, Pfeifer M. Enhanced ventilatory response to exercise in patients with chronic heart failure and central sleep apnea. Circulation 2003;107:1998-2003.
- Bradley TD, Logan AG, Kimoff RJ, Series F, Morrison D, Ferguson K, Belenkie I, Pfeifer M, Fleetham J, Hanly P, Smilovitch M, Tomlinson G, Floras JS, the CANPAP Investigators. Continuous positive airway pressure for central sleep apnea and heart failure. N Engl J Med 2005;353:2025-2033.


