A 61 year old female presented to an outside hospital with increasing shortness of breath and cough. She complained of a non-productive cough for approximately six weeks. She denied hemoptysis but complained of a low grade fever. Over this time she became progressively more short of breath. At the time of presentation she was able to only walk one hundred meters before she had to stop due to dyspnea.
Her past medical history included obesity, gastroesophageal reflux disease (GERD), peripheral vascular disease, hypertension, and type II diabetes. Family history was negative for lung cancer or chronic obstructive pulmonary disease (COPD). Her medications included aspirin, metoprolol, lisinopril, insulin glargine and esomeprazole. She denied any previous tobacco, alcohol or intravenous drug use. She was currently disabled due to chronic lower back pain.
Physical Exam
Her vital signs included a temperature of 101° F, respiratory rate of 28, blood pressure of 152/91 and heart rate of 99/min. Oximetry was 87% on room air. Physical exam revealed an obese female in mild respiratory distress. No accessory muscle use was noted. Right sided lung fields were clear. Left sided lung fields were clear posteriorly but diminished anteriorly. Cardiac exam was normal. No palpable lymphadenopathy was appreciated in the supraclavicular or axillary regions. The rest of the exam was unremarkable.
Lab
She presented to an outside hospital emergency department and was found to have an abnormal chest x-ray. Posterior-anterior (PA) and lateral films were provided (Figures 1 and 2).
Figure 1. Posterior-anterior chest x-ray demonstrating left sided consolidation without volume loss.
Figure 2. Lateral view on chest x-ray demonstrating left upper lobe consolidation.
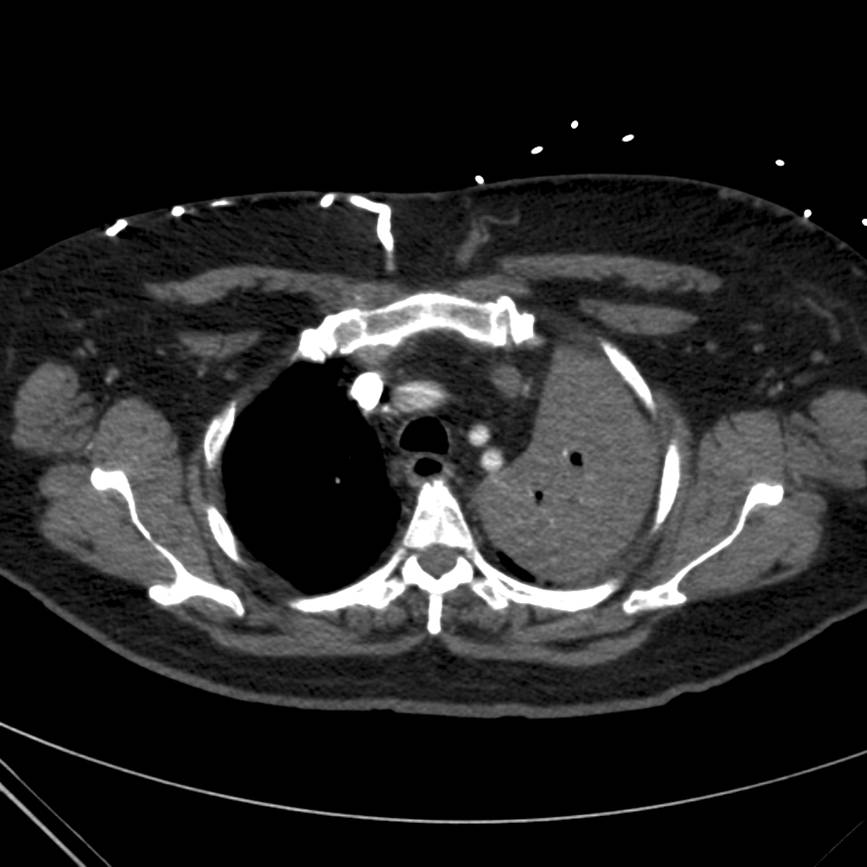
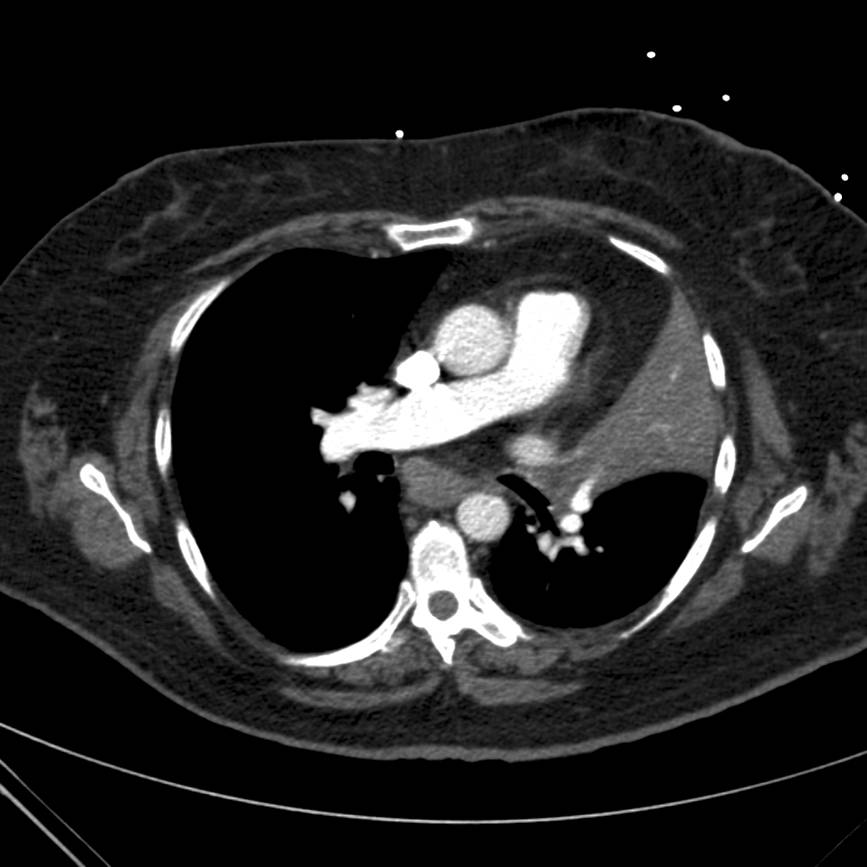
Subsequently the patient underwent computed tomography (CT) of the chest with pulmonary angiography. Two cuts are provided below (Figures 3 and 4).
Figure 3. Computed tomography image of the chest demonstrating consolidation of the left upper lobe.
Figure 4. Computed tomography image of the chest demonstrating left upper lobe (LUL) consolidation with endobronchial lesion in LUL bronchus.
The patient was admitted to the outside hospital and underwent bronchoscopy for evaluation of left upper lobe (LUL) and lingular collapse. She was electively intubated for the procedure and bronchoscopy revealed an endobronchial lesion in the LUL. The patient was transferred on mechanical ventilation to a tertiary care center for further evaluation of suspected endobronchial malignancy. Repeat bronchoscopy was performed with results as shown in Video 1.
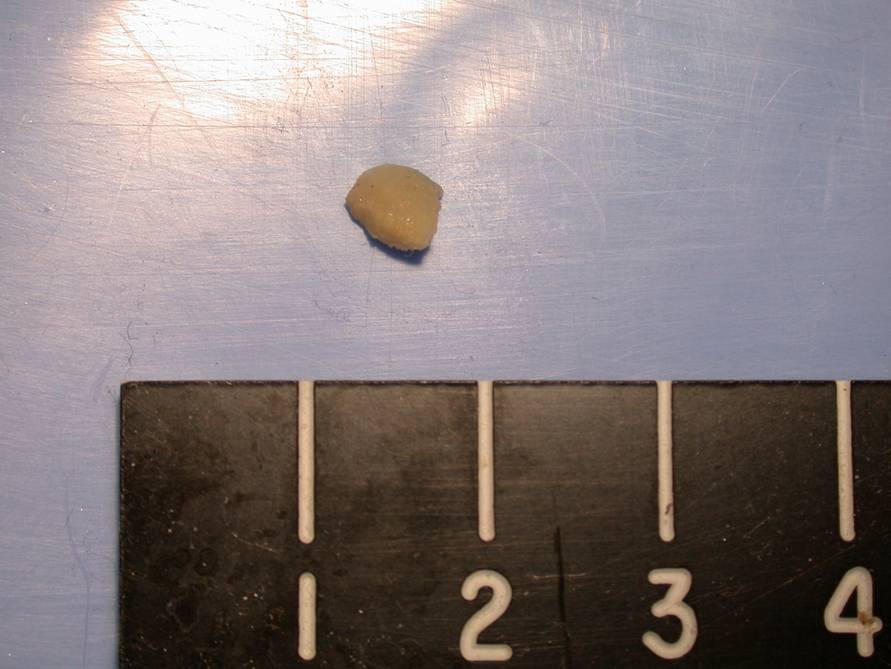
Bronchoscopy revealed a foreign body in the left upper lobe bronchus. Using cryotherapy, the foreign body was successfully removed and eventually identified as a popcorn kernel (Figure 5).
Figure 5. Foreign body identified as popcorn kernel.
C. Clinically, aspirated foreign bodies may commonly be confused with endobronchial malignancies based on the similar radiographic findings and initial gross appearances. Surrounding granulation tissue and secretions can obscure the margins making it difficult to correctly identify the nature of the obstructing lesion.
Foreign body aspiration is detailed extensively in children but less frequently in adults. The significance of the problem in adults is not minimal. In 2004, choking remained the fourth leading cause of unintentional injury or death in the United States and 4,100 deaths (1.4 deaths per 100,000 population) from unintentional ingestion or inhalation of food or other objects resulting in airway obstruction were reported[1]. The incidence rate in adults increases with age beginning in the sixth decade (2.6 deaths per 100,000 population aged 65-75 y) and rises rapidly after age 70 years (13.6 deaths per 100,000 population older than 75 y). Café coronary syndrome has been defined as the aspiration of a foreign body leading to immediate asphyxiation and death[2]. The incidence has been described at 0.66 per 100000. Since the angles made by the mainstem bronchi with the trachea are identical until 15 years of age foreign bodies are found on either side with equal frequency in children. After age 15 the right mainstem bronchus has a more acute angle off the trachea and foreign bodies are more commonly encountered here. Predisposing factors that have been described in previous reviews include primary neurologic disorders that result in impaired cough and swallowing, poor dentition, trauma, and sedative use[3]. Less common but still pertinent factors described are cultural practices such as not using eating utensils.
With further questioning, this patient remembered an incident of choking while eating popcorn lying on her couch approximately two months prior to presentation.
B. Infrequently (less than 50% of the time) - In his review, Lan divided patients into clinical categories of acute or chronic aspirated foreign bodies[4]. In acute aspiration, patients can present immediately with a discrete choking episode and respiratory symptoms of dyspnea, coughing, localized wheezing, or absent breath sounds. Penetration syndrome is the presence of intractable cough and choking with or without vomiting that occurs at the time of the event[5]. This has been reported to occur upward of 49% in cases of foreign body aspiration. For patients identified as having chronic aspiration, a discrete episode of choking was not often recalled[4]. In Lan’s review, the duration of foreign body presence in the lung was approximately 25 months. Clinical characteristics associated with chronic foreign body aspiration were refractory asthma symptoms with localized wheezing, delayed resolution of pneumonia with appropriate treatment or recurrent pneumonias. Clinical sequelae in the chronic group included bronchiectasis, hemoptysis or bronchial stricture.
D. - The initial tests to obtain are AP and lateral neck films, inspiratory and expiratory PA chest films and a lateral chest film. Lateral neck views may show swelling or infraglottic opacity[5]. Many of the x-ray findings are dependent upon the length of time that the foreign body has been present and the properties of the foreign body itself. Radiopaque materials such as metal or teeth are easily identified. Organic materials including bones may not be easily seen. Bones from cod, haddock and salmon are radioapaque while trout, mackerel, and herring bones are radiolucent[6]. Some foreign bodies may have a physiologic ball and valve effect on the expiratory film, resulting in hyperinflation during expiration on the affected side[7]. In chronic foreign body aspiration atelectasis is more often seen. Recurrent pneumonias with volume loss are a common presentation of chronic foreign body aspiration[4]. The diagnostic accuracy, sensitivity, and specificity of foreign body detection on chest x-rays was 67%, 68%, and 67%, respectively in one series 34 pediatric cases[8]. Chest computed tomography (CT) in the evaluation of foreign body in adults has been described in the literature but there are no large series that have provided the sensitivity or specificity of CT. CT scans offer the additional ability to detect the foreign body in the lumen of the tracheobronchial tree[9]. Sensitivity may be increased with the use of higher resolution CT scans. Typical findings include hyperlucency, lobar consolidation, bronchiectasis and atelectasis.
B. With regards to removal of the foreign body both flexible bronchoscopy and rigid bronchoscopy can be utilized. In one case series 90% of tracheobronchial foreign bodies were able to be removed using flexible bronchoscopy and 97% using the combination of the two procedures[10]. Cryotherapy can be useful in the removal of soft material as was the case here. Other tools that can be utilized with the flexible bronchoscope include forceps and basket retrieval devices. The nature of the foreign body is important to the clinical presentation and its subsequent removal. The foreign body reaction within the airway tends to be much stronger with vegetative materials than non-vegetative[11]. After becoming lodged vegetable material may swell over hours or days, worsening the obstruction. Oily nuts such as peanuts have been shown to induce significant congestion and edema due to the free fatty acid released from decomposition of the nut itself. Inert objects such as bone or metal often do not cause significant airway obstruction but tend to be sharper and can lend to bleeding on removal.
After the foreign body removal bronchoalveolar lavage (BAL) from the LUL stained positive for a beaded gram positive bacilli that was modified Ziehl-Neelson acid fast stain negative. Poor growth was noted in aerobic culture but granules were seen on examination of the biopsy material.
C. Actinomyces is classically defined by the aforementioned staining characteristics and lack of growth on aerobic media[12]. Culturing material from foreign bodies requires special care. Laboratory personnel should be alerted of the possibility of aerobic and anaerobic organisms along with the possible need for the use of special culture media. Cultures should be allowed to grow for extended periods due to the relatively slow growth of these organisms. The cultures should also be kept after initial identification of more common airway organisms in an attempt to visualize fastidious organisms.
The three members of the genera actinomycetes are Actinomyces, Nocardia and Streptomycoses. The Actinomyces species are nonspore forming anaerobic prokaryotic bacteria. The presence of gram positive bacilli with beaded, branched morphology are suggestive of actinomycoses. It will typically stain acid fast negative. Sulphur granules have classically been associated with these organisms. Risk factors include alcoholism and poor dentition with weaker evidence suggesting immunosuppression as a risk factor[12]. Clinically this is often confused with a malignancy due to its slow growing characteristics. It is often associated with malignancy as it tends to colonize dead tissue which may be seen with necrotic endobronchial malignancies. Diagnosis should include a combination of positive culture, demonstration of sulphur granules in purulent matter from infected tissue, correlation with the clinical and radiological features, and the response to antibiotic treatment. Actinomyces has been associated with foreign body aspiration in a previous case report[13]. Treatment consists of high dose intravenous penicillin for 2-6 weeks and then oral therapy for 6 to 12 months.
Differentiating amongst the members of the genera can be difficult as all have been associated with human disease. Nocardia species is identified as an aerobic, gram positive rod that stains partially acid fast[14]. This organism rarely forms granules and can be treated with trimethoprim/sulfamethoxazole. Streptomyces species typically cause mycetomas. They will often appear as an aerobic, gram positive rod. Acid fast staining is negative and these organisms often will produce granules. Treatment is also with trimethoprim /sulfamethoxazole.
Conclusion The patient was treated with IV penicillin and transitioned to oral therapy. At time of follow up she had radiographic resolution of her LUL collapse. Her cough had disappeared and she was back to her functional baseline.
References
National Safety Council, R.a.S.D. Injury Facts 2008 Edition, ed. N.S. Council. Vol.:8. 2008: Itasca, Ill.
Wick R.,Gilbert J.D., Byard R.W. Cafe coronary syndrome-fatal choking on food: an autopsy approach. J Clin Forensic Med 2006;13(3):135-8.
Limper A.H., Prakash U.B. Tracheobronchial foreign bodies in adults. Ann Intern Med 1990;112(8):604-9.
Boyd M., Chatterjee A., Chiles C, Chin R. Tracheobronchial Foreign Body Aspiration in Adults. Southern Medical Journal 2009;102(2):171-174.
Ell S, Sprigg A. The radio-opacity of fishbones — Species variation. Clinical Radiology 1991;44:104-107.
Esclamado RM. Laryngotracheal foreign bodies in children: A comparison with bronchial foreign bodies. Am J Dis Child 1987;141(3):259-62.
Svedström E, Kero P. How accurate is chest radiography in the diagnosis of tracheobronchial foreign bodies in children? Pediatr Radiol. 1989;19(8):520-2.
Zissin R, Shapiro-Feinberg M, Rozenman J, Apter S, Smorjik S, Hertz M. CT findings of the chest in adults with aspirated foreign bodies. Eur Radiol. 2001:11(4):606
Debeljak A, Sorli J, Music E, Kecelj P. Bronchoscopic removal of foreign bodies in adults: experience with 62 patients from 1974-1998. Eur Respir J.1999;4(4):792-5.
Takako H. Supplemental experimental findings on foreign body in the bronchus. J Jpn Bronchoesophagol Soc. 1973;24:30-39.
Mabeza G.F., Macfarlane J. Pulmonary actinomycosis. Eur Respir J. 2003; 21:545-551.
Walters G, Ware N, Handslip P.Endobronchial actinomycosis associated with aspiration of a shirt button: A 30-year latency. Respiratory Medicine CME 2009 Vol. 2, Issue 1, Pages 18-20, DOI: 10.1016/j.rmedc.2008.10.018.
Rippon JW. Medical Mycology. Inc. Wonsiewicz MJ, ed. The Pathogenic Fungi and the Pathogenic Actinomycetes. 3rd edn. Philadelphia. W.B. Saunders Co., 1988; pp. 30-52.
The American Thoracic Society improves global health by advancing research, patient care, and public health in pulmonary disease, critical illness, and sleep disorders. Founded in 1905 to combat TB, the ATS has grown to tackle asthma, COPD, lung cancer, sepsis, acute respiratory distress, and sleep apnea, among other diseases.
AMERICAN THORACIC SOCIETY 25 Broadway New York, NY 10004 United States of America