Persistent Dyspnea in a Patient with Down’s Syndrome
Reviewed By Allergy, Immunology & Inflammation Assembly
Submitted by
Sindhu Mukku, MD
Fellow
Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
The Ohio State University Wexner Medical Center
Columbus, Ohio
S. Patrick Nana-Sinkam, MD
Associate Professor of Internal Medicine
Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
The Ohio State University Wexner Medical Center
Columbus, Ohio
Submit your comments to the author(s).
History
A 21-year old man with Down’s Syndrome presented from an outside hospital with the complaint of three weeks of persistent cough and dyspnea. Prior to seeking care at our facility, he was treated at a local community hospital for progressively worsening cough, productive of thick yellow sputum. He was started on broad-spectrum antibiotics, prednisone, and bronchodilators. Computed Tomography (CT) of the chest revealed bibasilar atelectasis and apical emphysematous changes. He also underwent a bronchoscopy, which revealed thick secretions, but was otherwise unremarkable with negative bacterial cultures.
He was subsequently transferred to our institution for further evaluation and upon arrival, complained of sinus congestion, post-nasal drip, and cough productive of foul-smelling sputum.
Past Medical and Surgical History: Trisomy 21, diabetes mellitus, alpha-1 antitrypsin carrier (MZ phenotype), and repair of patent ductus arteriosus as a child.
Family and Social History: Mother is an alpha-1 antitrypsin carrier (MZ phenotype). Patient denied cigarette, alcohol, or illicit drug use, but was exposed to mother’s second-hand smoke. He had no known exposures to farm-animals, birds, or tuberculosis.
Physical Exam
He was a well-developed male in moderate respiratory distress. His oxygen saturation on 6 liters via nasal cannula was 95%. His temperature was 37 C, respiratory rate 26, heart rate 110 beats per minute, and blood pressure 112/75. He had no palpable sinus tenderness. Oral exam revealed a grade 3 Mallampati airway. He had a barking cough that could be heard throughout the corridors. There were diminished sounds at the lung bases but otherwise no wheezing, rhonchi, or rales. Physical exam was otherwise unremarkable.
The patient was placed on broad-spectrum intravenous antibiotics. Sputum was sent for culture and showed heavy purulence but no organisms. Serologies were sent for Bordatella pertussis and Legionella, which were negative.
Figures

Figure 1. Chest Radiograph showing generally clear lung fields without obvious focal airspace disease.
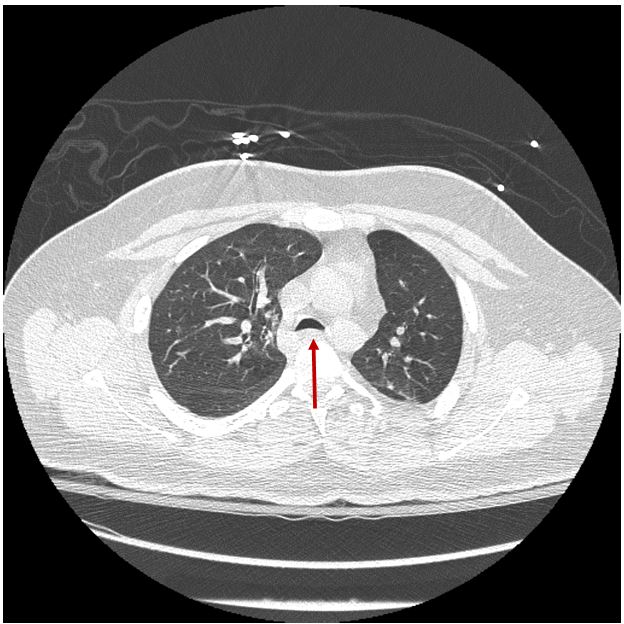
Figure 2.1 Computed Tomography (CT) of the chest showing decreased anterior-posterior diameter of the tracheal lumen
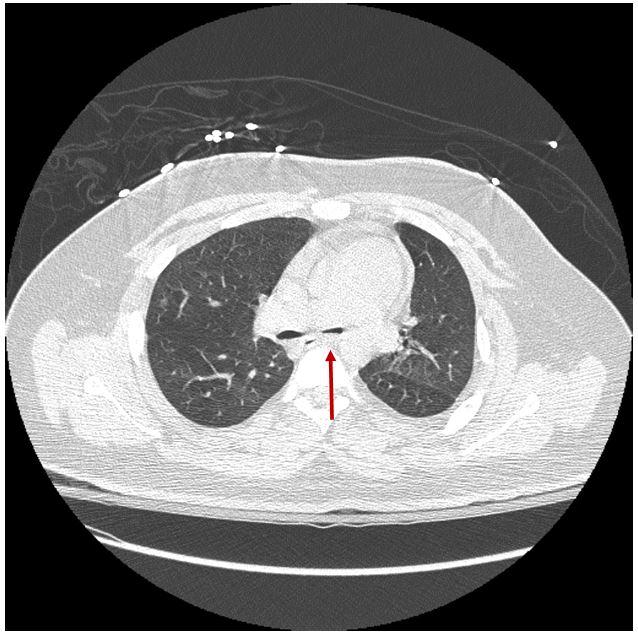
Figure 2.2 CT of the chest showing significant luminal collapse at the level of the carina
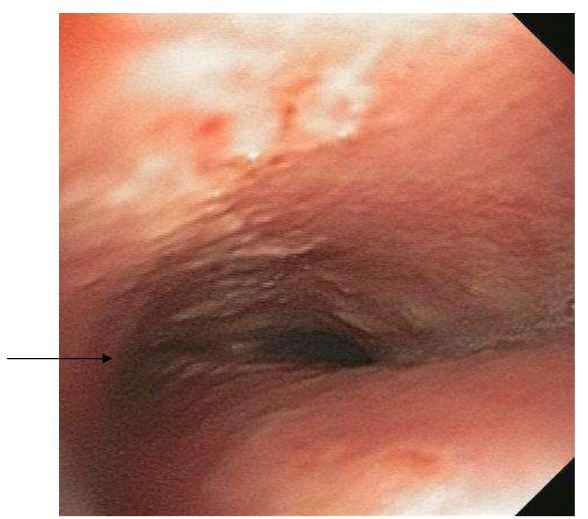
Figure 3. Photo taken during bronchoscopy demonstrating abnormal appearance of tracheal wall and cartilaginous rings at the level of the carina. Note the relative flattening of the left mainstem bronchus compared to the right.
Answer: C
Respiratory problems are the most common reason for children with Down’s Syndrome to be admitted to the hospital and are an important cause of mortality. Developmental abnormalities such as hypotonia, craniofacial anomalies, and cardiac anomalies contribute to the development of respiratory disease.1 All of the above conditions, except for bronchopulmonary dysplasia, are more commonly seen in children with Down’s Syndrome than in the general pediatric population.
Studies have shown that various immunoglobulin deficiencies may contribute to the development of recurrent respiratory infections.1 Developmental delay of the oropharyngeal structures and relative tongue enlargement are implicated in chronic aspiration pneumonia as well. Obstructive sleep apnea is more frequently seen in children with Down’s Syndrome due to narrower nasal airways, micrognathia, increased collapsibility of the oropharyngeal and hypopharyngeal airway, and large tongue.2 Children with Down’s Syndrome are also at risk of development of pulmonary arterial hypertension because of the increased frequency of intra-cardiac right-to-left shunts, which leads to increased pulmonary blood flow. Finally, tracheobronchomalacia is commonly seen in children with Down’s Syndrome due to developmental abnormalities of the tracheal rings. Bronchopulmonary dysplasia is a condition seen in neonates and is associated with prematurity, respiratory failure, oxygen supplementation, and mechanical ventilation, but is not associated with Down’s Syndrome.
Answer: B
Tracheomalacia and tracheobronchomalacia refer to collapsibility of the tracheal and bronchial walls due to weakness.3 They occur during expiration and are most apparent on forced expiratory maneuvers such as cough and Valsalva maneuver. Tracheal collapse during coughing often makes clearance of secretions difficult. Common symptoms include a barking seal-like cough, recurrent respiratory tract infections, orthopnea, dyspnea, and wheezing.
Tracheobronchomalacia can be divided into congenital (primary) forms, and acquired, (secondary) forms. Congenital causes of tracheobronchomalacia are thought to be due to developmental abnormalities of the collagen matrix. Numerous congenital conditions are associated with tracheobronchomalacia, including Down’s Syndrome, tracheo- esophageal fistula, and bronchopulmonary dysplasia. Prematurity is also a risk factor for tracheobronchomalacia, likely due to the immature collagen in the tracheal rings.
Secondary or acquired causes of tracheobronchomalacia are more common. Prolonged endotracheal intubation and tracheotomy are the most common causes of acquired focal tracheomalacia in adults. One potential mechanism includes compromise of tissue blood supply secondary to cuff pressures thereby causing destruction of the supporting cartilage and subsequent weakening of the tracheal wall.3 Chronic inflammatory conditions such as relapsing polychondritis, chronic obstructive pulmonary disease and gastroesophageal reflux disease (with chronic aspiration) are also important risk factors for development of airway malacia.
Extrinsic compression of the trachea can also cause tracheomalacia. Examples include vascular compression (double aortic arch, abnormal take-off of the innominate artery, vascular rings), compression from tumors (bronchogenic cysts, teratomas), and skeletal abnormalities (scoliosis, pectus excavatum). Obesity is not considered to be a cause of extrinsic compression causing tracheomalacia. Excess weight on the anterior chest wall due to obesity, however, lowers chest wall compliance and respiratory muscle endurance. While collapse of the upper airway and subsequent obstructive sleep apnea is associated with obesity, collapse of the lower airways is generally not associated with obesity.
Answer: C
The gold standard for diagnosis of tracheomalacia is direct visualization with of tracheal narrowing by bronchoscopy of at least 50% in the sagittal plane.3,4 However, multi-detector CT is being more frequently used as a non-invasive method of detecting tracheobronchomalacia in patients with a high index of clinical suspicion. Its non-invasive nature is especially attractive in the pediatric population. Traditionally, the paired end-inspiratory and end-expiratory CT technique has been used. This technique is recommended for those patients that are unable to follow dynamic breathing instructions. However, one concern with this technique is that tracheal collapse is submaximal at end-expiration. CT imaging while coughing is reported to produce a greater degree of collapse compared with forced expiration, but this method is believed to lead to over diagnosis of tracheomalacia. The paired end-inspiratory and dynamic expiratory technique is the preferred method for CT detection of tracheomalacia. The patient is instructed first to inhale deeply (to inspiratory capacity) and hold for image acquisition. They are then instructed to exhale, during which time dynamic CT images are acquired.5 In a recent comparison between dynamic expiratory and end-expiratory techniques, tracheomalacia was more frequently detected with dynamic acquisition of images at a variety of threshold levels.5 Comparison of dynamic expiratory CT and bronchoscopy showed a high degree of concordance for the detection of airway malacia.
Answer: A
Treatment of tracheomalacia is largely based on the patients’ symptom burden and the severity of the tracheal collapse. If asymptomatic, then no treatment is warranted. CPAP is the preferred non-invasive treatment of choice, as it acts as a pneumatic stent. CPAP can be worn intermittently during the day and night and can facilitate clearance of secretions.3 For tracheomalacia caused by vascular anomaly and compression, aortopexy is the procedure of choice. In this procedure, traction sutures are placed in the ascending aorta to pull the anterior wall of the trachea forward. The mechanical fixation of the aorta widens the anterior-posterior dimensions of the trachea and prevents collapse.
Metal stents have been successfully used for tracheal stenosis due to non-benign diseases of the airway; complications have limited their use in benign disorders. However, complications include granulation tissue formation, mucous plugging, stent migration, and difficult retrieval. In 2005, the Food and Drug Administration released a public health notification regarding serious complications from the use of metallic stents for benign diseases of the airway, including tracheomalacia. Silicone stents appear to have fewer complications and are an option for treatment in patients with severe symptoms or those who need a bridge to surgical correction of the abnormality. Tracheoplasty is a surgical option reserved for severe cases that do not respond to other modalities. It involves plication of the posterior membranous wall of the trachea with a polypropylene mesh to reinforce the airway and recreate the normal airway shape. In 2011, Ernst et al. showed that airway stabilization with silicone stent and/or tracheobronchoplasty led to improvement in the St. George Respiratory Questionnaire and the Health Related Quality of Life questionnaire.6
Tracheostomy may be effective if the tracheostomy tube bypasses the collapsed segment and splints the airway. However, more distal collapse will not be splinted with a tracheostomy alone. Tracheostomy can provide access for treatment with positive-pressure ventilation to maintain an open airway. In the pediatric population, tracheostomy can aggravate the underlying tracheomalacia and is therefore not the first line treatment.3
Answer: C
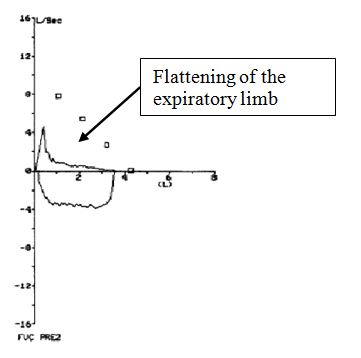
All of the above are potential long term complications of tracheomalacia except for development of restriction on PFTs. In fact, there is limitation on the expiratory component, which leads to an obstructive pattern on the PFTs. PFTs can also show reduced mid- expiratory/mid-inspiratory ratio, as below.3 The flow-volume loop may show flattening due to the collapse of the trachea on expiration. Tracheal and bronchial collapse during coughing leads to decreased ability to clear secretions and can thereby lead to recurrent respiratory tract infections and, in severe cases, respiratory failure.
References
- McDowell KM, Craven DI. Pulmonary complications of Down syndrome during childhood. J Pediatr. 2011 Feb;158(2):319-25. Epub 2010 Sep 16. Review. PubMed PMID: 20846671.
- Pandit C, Fitzgerald DA. Respiratory problems in children with Down syndrome. J Paediatr Child Health. 2012 Mar;48(3):E147-52. doi: 10.1111/j.1440-1754.2011.02077.x. Epub 2011 Apr 29. Review. PubMed PMID: 21535288.
- Carden KA, Boiselle PM, Waltz DA, Ernst A. Tracheomalacia and tracheobronchomalacia in children and adults: an in-depth review. Chest. 2005 Mar;127(3):984-1005. Review. PubMed PMID: 15764786.
- Lee KS, Sun MR, Ernst A, Feller-Kopman D, Majid A, Boiselle PM. Comparison of Dynamic Expiratory CT With Bronchoscopy for Diagnosing Airway Malacia: A Pilot Evaluation. Chest. 2007 Mar;131(3):758-64. PubMed PMID: 17356090.
- Ferretti GR, Jankowski A, Perrin MA, Chouri N, Arnol N, Aubaud L, Pepin JL. Multi-detector CT evaluation in patients suspected of tracheobronchomalacia: comparison of end-expiratory with dynamic expiratory volumetric acquisitions. Eur J Radiol. 2008 Nov;68(2):340-6. Epub 2007 Oct 29. PubMed PMID: 17913426
- S, Michaud G, Herth F, Ernst A. Tracheobronchoplasty for severe tracheobronchomalacia: a prospective outcome analysis. Chest. 2008 Oct;134(4):801-7. PubMed PMID: 18842912.


