Acute Respiratory Distress Syndrome Secondary to an Unusual Infection
Reviewed By Microbiology, Tuberculosis & Pulmonary Infections Assembly
Submitted by
Carmen Luraschi-Monjagatta, M.D.
Fellow
Division of Pulmonary and Critical Care Medicine
University of Arizona
Tucson, Arizona
Linda Snyder, M.D.
Professor of Medicine
Division of Pulmonary and Critical Care Medicine
University of Arizona
Tucson, Arizona
Submit your comments to the author(s).
History
A 39 year-old man from Whiteriver, Arizona presented to the Emergency Department with a five-day history of fever, chills, nausea, vomiting, and cough productive of purulent sputum. He had evidence of acute kidney injury and sepsis and was transferred to our hospital for further evaluation. Upon admission to our hospital, he had diffuse abdominal pain with diarrhea, left foot pain, cough and mild dyspnea.
Past medical history is significant for poorly controlled diabetes mellitus, severe peripheral vascular disease with previous toe amputations, hypertension, hyperlipidemia and depression.
Social history is notable for previous alcohol abuse and a 50 pack-year smoking history. He lives on the Apache Indian Reservation and denied recent travel. He denied recreational drug use.
Medications include gabapentin, atenolol, simvastatin, aspirin, glypizide, pioglitazone, sertraline and trazodone. Prior to transfer, he was given clindamycin for presumed pneumonia and sepsis.
Physical Exam
Vital signs revealed a temperature 38.8°C, blood pressure 163/93 mmHg, heart rate 92 beats per minute, respiratory rate 24 breaths per minute, and oxygen saturation 94% on 4L oxygen by nasal cannula. The patient was in moderate respiratory distress. Cardiac examination revealed a regular rate and rhythm without murmurs or gallop. Respiratory examination revealed diffuse inspiratory crackles without wheezing. The abdomen was non-tender and non-distended, without hepatosplenomegaly. Extremities revealed a right leg ulcer without signs of infection, but no clubbing. He had no rash.
Lab
Complete blood count showed a white blood cell count of 13,100/ml with 66% neutrophils, 24% basophils, 7% lymphocytes, 3% monocytes, 0% eosinophils, hemoglobin 13 g/dl, hematocrit 36% and platelet count of 85,000/ml.
Comprehensive metabolic panel demonstrated: sodium 127 mMol/L, potassium 3.2 mMol/L, chloride 98 mMol/L, bicarbonate 19 mMol/L, blood urea nitrogen 26 mg/dl, creatinine 2.7 mg/dl, glucose 192 mg/dl, total protein 6.6 mg/dl, albumin 1.7 g/dl, bilirubin 0.6 mg/dl, AST 71IU/L, ALT 72 IU/L, and alkaline phosphatase of 99 UI/L.
Arterial lactate was 4.3 mmol/L (normal lactate: < 2 mmol/L) and C-reactive protein (CRP) was 21.9 mg/dl (normal CRP: < 1mg/dl).
Radiographic Studies
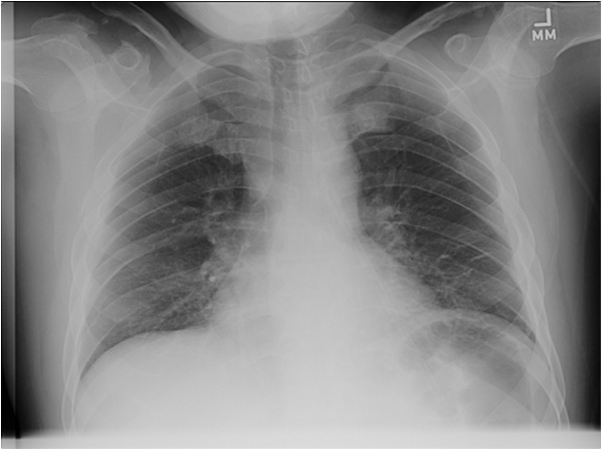
Figure 1: Chest radiograph on admission to our hospital
Hospital course
The patient was treated for sepsis and severe community acquired pneumonia with empiric piperacillin- tazobactam and vancomycin. Over the next two days, the patient’s respiratory status worsened and he required intubation and mechanical ventilation. Chest radiographs showed bilateral diffuse pulmonary infiltrates consistent with acute respiratory distress syndrome (ARDS) (Figure 2). Bronchoscopy with bronchoalveolar lavage revealed no evidence of alveolar hemorrhage, cell count with 65% neutrophils, 26% lymphocytes and 9% macrophages and cytology and all cultures were unrevealing. HIV serology was negative. Legionella urinary antigen was negative. The subsequent physical examination showed a petechial rash on the lower extremities.
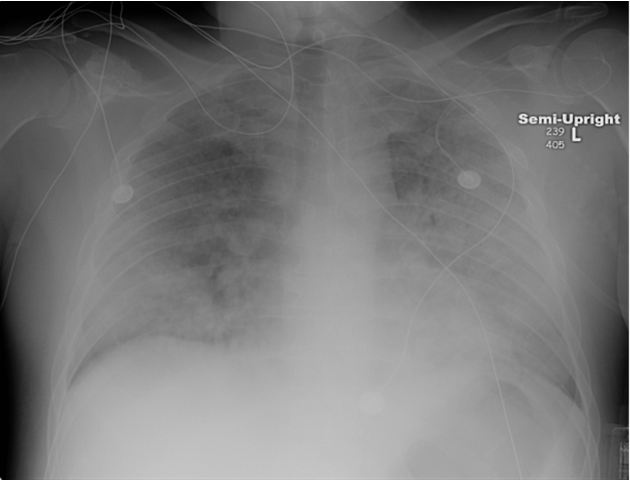
Figure 2: Chest radiograph in the Intensive Care Unit
Serologic testing for rickettsial infection
Based on epidemiological suspicion and the evolving clinical scenario, the patient was initiated on an additional antibiotic and rickettsial serologies were sent. The patient’s serologic tests for rickettsial infection were elevated with an IgM 1: 256 and IgG 1: 256. A follow-up IgG titer was elevated at 1: 2048, which confirmed the diagnosis of Rocky Mountain spotted fever (RMSF). The patient fully recovered.
RMSF is a life-threatening, tick-borne disease caused by Rickettsia rickettsii. It is the most common rickettsial infection in the United States. Only 70% of patients have a history of a tick bite or exposure. The incubation period is 3-12 days. The diagnosis is usually confirmed with serologic testing. Treatment decisions must not be delayed awaiting serologic tests because early empiric antibiotic therapy can prevent morbidity and death. Patients with RMSF may not have the rash when they initially seek medical care during the first 2-5 days of the illness.
The diagnosis must be made based on clinical and laboratory findings and epidemiological information. Clues to the diagnosis are occupational or recreational activities, tick exposures and epidemiological data (1). Serologic testing for RMSF is done using indirect immunofluorescence antibody (IFA) assay, which is quantitative and considered to be the gold standard, or enzyme-linked immunosorbent (ELISA) assay. Two sequential serum samples demonstrating a rising IgM or IgG antibody titer are crucial to confirm acute infection. It is important to note that serologic testing is dependent on the timing of collection of the sample and antibody titers are typically negative in the first week of the disease, hence negative serologic tests during this time do not exclude RMSF (1, 2). Therefore, empiric treatment for RMSF cannot be delayed. The sensitivity of the IFA assay is 94 to 100% after 14 days.
Two additional methods for diagnosis are should be noted. Amplification of specific DNA by PCR may detect rickettsial infections and is available in from the CDC and research laboratories (1). PCR is felt to be more useful for detecting rickettsial organisms in a skin biopsy or autopsy specimen. In addition, immunohistochemical staining of a biopsied skin lesion may be useful for RMSF diagnosis in patients who have not yet developed antibody titers.
Culture techniques are not used for RMSF diagnosis due to safety issues and are performed only in reference laboratories. Microscopic examination of blood smears is not useful to diagnosis of RMSF.
Infection of endothelial cells in blood vessels causing vasculitis
Rickettsia rickettsii is a weakly gram-negative coccobacillus in the genus Rickettsia. It is an obligate intracellular pathogen that uses substrates of the host cell to survive, and is transmitted by tick species, which are the vectors for RMSF (1,7). In the United States, the most common ticks implicated are the Rocky mountain wood tick (Dermacentor andersoni), American dog tick (Dermacentor variabilis), and the brown dog tick (Rhipicephalus sanguineus), a new vector from Arizona implicated in 2005, (1,3).
Rickettsia rickettsii infect endothelial cells of small and medium size vessels, which leads to increased vascular permeability and capillary leakage. This results in diffuse vascular damage, hemorrhage and necrosis known as rickettsial vasculitis (8,9).
The pathophysiology of ARDS in RMSF is multifactorial. Pulmonary edema may be due to capillary leakage caused by direct pulmonary involvement or a component of cardiogenic pulmonary edema from rickettsial vasculitis of the coronary arteries. In addition, neurologic involvement with cerebral edema may lead to neurogenic pulmonary edema. The microorganism has been observed in the alveolar septa and vascular endothelium and walls resulting in edema, septal congestion, interstitial pneumonia and hemorrhage (6).
The clinical presentation of RMSF is usually one of a systemic illness and may include fever, chills, headache, myalgia, malaise, nausea, and vomiting. These symptoms are nonspecific and lead to diagnostic challenges for clinicians. The incubation period varies from 2 to 14 days. In RMSF, a rash typically appears 2 to 4 days after the onset of fever. However, rash might be absent or atypical in up to 20% of RMSF cases. If present, lesions are typically macular rose-colored blanching lesions, petechiae, or ecchymoses on the extremities (1,2). Rash is not pathognomonic and can occur in other illnesses or infections. It can involve the entire body, including the palms and soles or it can be evanescent and localized to one region of the body.
RMSF is a multisystem disease and many organs can be affected as a result of the generalized vasculitis. Neurologic manifestations are common and include headache, delirium and meningoencephalitis. Disseminated intravascular coagulation results in thrombocytopenia and anemia. Acute kidney injury and hepatitis can occur. Pneumonitis due to infection of the pulmonary microcirculation can occur and lead to ARDS.
The patient in this case was initiated on doxycycline 100mg IV twice daily. The treatment of choice for RMSF is a tetracycline-class antibiotic, specifically doxycycline. Intravenous therapy is indicated for hospitalized patients. The drug is bacteriostatic in its activity against rickettsial organisms. The recommended dose is 100 mg twice daily (intravenously or orally) for adults. The optimal duration of treatment has not been established but current recommendations suggest therapy for at least three days after the fever resolves and clinical improvement is noted, typically 5-7 days. Severe multi-organ involvement may require a longer course of treatment. Chloramphenicol is an alternate therapy that has been used to treat RMSF. However, epidemiologic data suggest patients with RMSF treated with chloramphenicol have a higher mortality than those who receive a tetracycline (1).
References
- Chapman AS, Bakken JS, Folk SM, Paddock CD, Bloch KC, Krusell A, Sexton DJ, Buckingham SC, Marshall GS, Storch GA, Dasch GA, McQuiston JH, Swerdlow DL, Dumler SJ, Nicholson WL, Walker DH, Eremeeva ME, Ohl CA; Tickborne Rickettsial Diseases Working Group; CDC. Diagnosis and Management of Tickborne Rickettsial Diseases: Rocky Mountain spotted fever, Ehrlichioses, and Anaplasmosis--United States: A practical guide for physicians and other health-care and public health professionals. MMWR Recomm Rep. 2006 Mar 31; 55(RR-4): 1-27.
- Dantas-Torres F. Rocky Mountain spotted fever. Lancet Infect Dis. 2007; 7(11): 724-32.
- Demma LJ, Traeger MS, Nicholson WL, Paddock CD, Blau DM, Eremeeva ME, Dasch GA, Levin ML, Singleton J Jr, Zaki SR, Cheek JE, Swerdlow DL, McQuiston JH. Rocky Mountain spotted fever from an unexpected tick vector in Arizona. N Engl J Med. 2005; 353(6): 587-94.
- Gonçalves da Costa PS, Brigatte ME, Pereira de Almeida E, de Carvalho Valle LM. Atypical fulminant Rickettsia rickettsii infection (Brazilian spotted fever) presenting as septic shock and adult respiratory distress syndrome. Braz J Infect Dis. 2002; 6(2) :91-6.
- Memis D, Sapolya O, Tasdogan M, Yucel T, Vatan I. Rickettsia ricketsii infection presenting as septic shock and adult respiratory distress syndrome. Journal of Chinese Clinical Medicine. 2007,6: Vol 2 (6).
- Walker DH, Crawford CG, Cain BG. Rickettsial infection of the pulmonary microcirculation: the basis for interstitial pneumonitis in Rocky Mountain spotted fever. Hum Pathol. 1980; 11 (3): 263-72.
- Chen LF, Sexton DJ. What's new in Rocky Mountain spotted fever? Infect Dis Clin North Am. 2008; 22(3): 415-32, vii-viii.
- Sahni SK, Rydkina E. Host-cell interactions with pathogenic Rickettsia species. Future Microbiol. 2009; 4(3): 323-39.
- Walker DH, Valbuena GA, Olano JP. Pathogenic mechanisms of diseases caused by Rickettsia. Ann N Y Acad Sci. 2003; 990: 1-11.


